

Phase 1 dose-escalation study of SEA-CD40: a non-fucosylated CD40 agonist, in advanced solid tumors and lymphomas
- PMID: 37385724
- PMCID: PMC10314623
- DOI: 10.1136/jitc-2022-005584
Phase 1 dose-escalation study of SEA-CD40: a non-fucosylated CD40 agonist, in advanced solid tumors and lymphomas
Abstract
Background: SEA-CD40 is an investigational, non-fucosylated, humanized monoclonal IgG1 antibody that activates CD40, an immune-activating tumor necrosis factor receptor superfamily member. SEA-CD40 exhibits enhanced binding to activating FcγRIIIa, possibly enabling greater immune stimulation than other CD40 agonists. A first-in-human phase 1 trial was conducted to examine safety, pharmacokinetics, and pharmacodynamics of SEA-CD40 monotherapy in patients with advanced solid tumors and lymphoma.
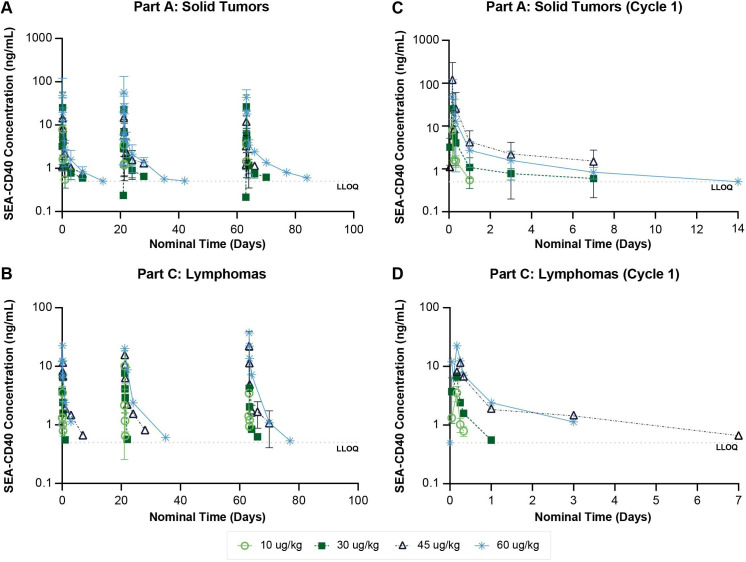
Methods: SEA-CD40 was administered intravenously to patients with solid tumors or lymphoma in 21-day cycles with standard 3+3 dose escalation at 0.6, 3, 10, 30, 45, and 60 µg/kg. An intensified dosing regimen was also studied. The primary objectives of the study were to evaluate the safety and tolerability and identify the maximum tolerated dose of SEA-CD40. Secondary objectives included evaluation of the pharmacokinetic parameters, antitherapeutic antibodies, pharmacodynamic effects and biomarker response, and antitumor activity.
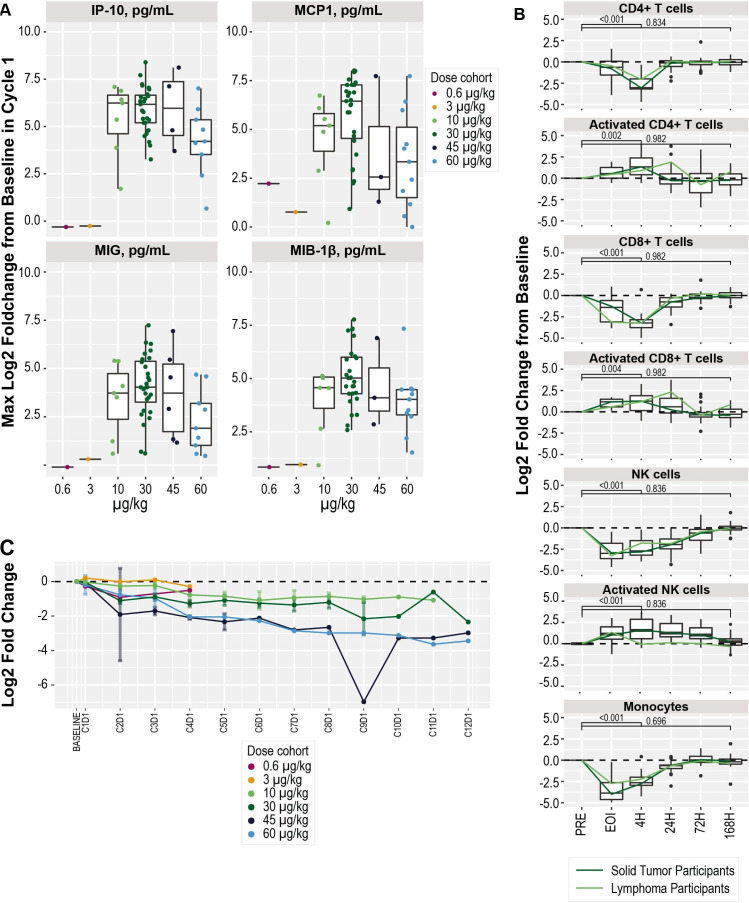
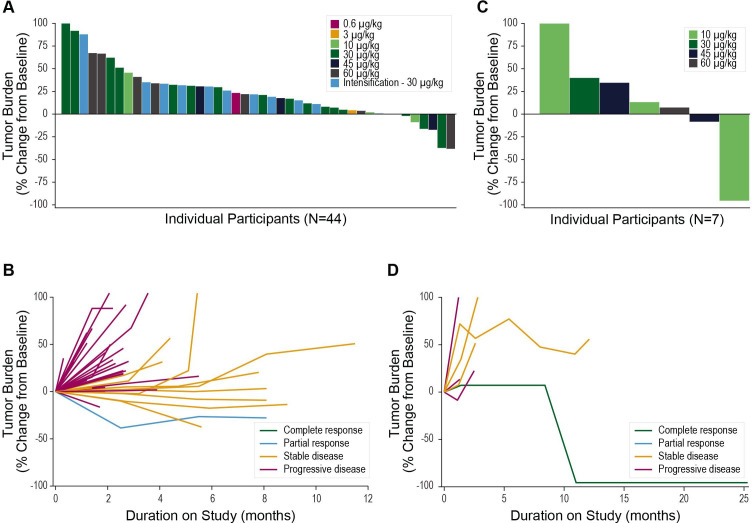
Results: A total of 67 patients received SEA-CD40 including 56 patients with solid tumors and 11 patients with lymphoma. A manageable safety profile was observed, with predominant adverse events of infusion/hypersensitivity reactions (IHRs) reported in 73% of patients. IHRs were primarily ≤grade 2 with an incidence associated with infusion rate. To mitigate IHRs, a standardized infusion approach was implemented with routine premedication and a slowed infusion rate. SEA-CD40 infusion resulted in potent immune activation, illustrated by dose dependent cytokine induction with associated activation and trafficking of innate and adaptive immune cells. Results suggested that doses of 10-30 µg/kg may result in optimal immune activation. SEA-CD40 monotherapy exhibited evidence of antitumor activity, with a partial response in a patient with basal cell carcinoma and a complete response in a patient with follicular lymphoma.
Conclusions: SEA-CD40 was tolerable as monotherapy and induced potent dose dependent immune cell activation and trafficking consistent with immune activation. Evidence of monotherapy antitumor activity was observed in patients with solid tumors and lymphoma. Further evaluation of SEA-CD40 is warranted, potentially as a component of a combination regimen.
Trial registration number: NCT02376699.
Keywords: antibodies, neoplasm; head and neck neoplasms; immunotherapy; lung neoplasms.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ALC reports receiving commercial research grants from Actuate, Abgenomics, Amgen, AstraZeneca, Novocure, Nucana, and Seagen. DCS reports receiving commercial research grants from Agensys, Atterocor/Millendo, Bayer, Bristol-Myers Squibb, Celgene, F. Hoffman-LaRoche, Incyte, Lilly, MedImmune/AstraZeneca, Millennium/Takeda, Novartis, OncoMed, Merck, Roche/Genentech, Seagen. TP reports receiving commercial research grants from AbbVie, Bayer, Bristol-Myers Squibb, Incyte, Celgene, Genentech; reports receiving honoraria from Lymphoma Connect; and is a consultant/advisory board member for AbbVie, ADCT Therapeutics, AstraZeneca, Bayer, Bristol-Myers Squibb/Celgene, Genentech, Gilead/Kite, Karyopharm, Incyte, Morphosys, Pharmacyclics, Seagen, and TG therapeutics. BDC reports receiving commercial research grants from Clinigen and Galectin Therapeutics; reports receiving honoraria from Merck, Nektar and Clinigen. SG reports receiving commercial research grants from Seagen. AM reports receiving commercial research grants from Incyte, Takeda, Forty Seven Inc/Gilead, Juno pharmaceuticals/Bristol-Myers Squibb, Celgene/Bristol-Myers Squibb, Oncotartis, Innate pharmaceuticals, Seagen, TG Therapeutics, Affimed, Merck, Kite/Gilead, Roche-Genentech, ADC therapeutics, Miragen, Rhizen Pharmaceuticals; reports consultant/advisory board member/speaker bureau for Gilead, AstraZeneca, Pharmacyclics, Seagen, Incyte, Morphosys/Incyte, TG Therapeutics, Carevive, Kyowa Kirin, and Rigel pharmaceuticals. TMK reports receiving commercial research grants from Seagen, Bristol-Myers Squibb, Esai, Soligenix, Jannsen, Pfizer, Exelixis; is a consultant/advisory board member/speaker bureau for Tyme, Merck Sharpe Dome, Amgen, Seagen, Engene, Exelixis, Novartis, Pfizer, Genomic Health, Sanofi, and Bristol-Myers Squibb. SNM was a site investigator for this study. Olivier Rixe reports receiving commercial research grants from Bexion, Kyowa Kirin, Newlink, Rgenix, Oxford biotherapeutics, Daiichi, and Seagen. DLB reports commercial research grants from Seagen, Astellas Pharma US, Rafael Pharmaceuticals, Immunicum AB, and TESARO. TFG reports commercial research grants from Roche-Genentech, Bristol-Myers Squibb, Merck, Incyte, Seagen, Celldex, Evelo, Bayer, Aduro, Pyxis; is a consultant/advisory board member for Roche-Genentech, Merck, AbbVie, Bayer, Jounce, Aduro, Fog Pharma, Adaptimmune, FivePrime, Pyxis, Allogene and holds ownership interest (including patents) in Jounce, Pyxis, Aduro, Evelo, Bristol-Myers Squibb. MG reports commercial research grants from Boehringer Ingelheim, Bristol-Myers Squibb, Checkpoint Therapeutics, Eisai, GSB Pharma, Incyte, Johnson & Johnson, MedImmune, Merck, Moderna Therapeutics, NextCure, Pfizer, Regeneron, Roche/Genentech, Sanofi, Seagen, Silenseed; reports receiving honoraria from Foundation Medicine, Guardant Health; and is a consultant/speaker bureau for Exenex, Bristol-Myers Squibb, Lilly, Merck. HJL reports receiving commercial research grants from Bristol-Myers Squibb, Celgene, Oncternal Therapeutics, Seagen, and Takeda; is a consultant/advisory board member/speaker bureau for Bristol-Myers Squibb, Guidepoint Global, and Aptitude Health. AKG reports receiving commercial research grants from Merck, I-Mab bio, IgM Bio, Takeda, Gilead, AstraZeneca, Agios, Janssen, Bristol-Myers Squibb, Seagen; is a consultant and receives honoraria from Incyte, Kite, Morphosys, ADC, Acrotech, Merck, Karyopharm, Nurix, Cellectar, Janssen, Seagen, Epizyme, I-Mab bio. PC reports receiving commercial research grants from Genetech, ADC Therapeutics; is a consultant/advisory board member/speaker’s bureau for Verastem, Seagen, Amgen, Kite, Bayer, TG Therapeutics, Celgene. EIH reports commercial research grants from Agensys, AIQ, Astellas, AstraZeneca, Bayer, Boehringer, Bristol-Myers Squibb, Calibr, Caris, Celgene, Celldex, Champions, Corcept, Curemeta, Daiichi Sankyo, Dendreon, eFFECTOR, Eisai, Esanik, Five Prime, Fortis, Genentech/Roche, GSK, Ignyta, Infinity, Inovio, Janssen; receives honoraria from AstraZeneca, Bayer, Dendreon, Sanofi, Seagen, is a consultant/speaker bureau for Agensys, AstraZeneca, Bayer, Caris Centers of Excellence, Dendreon, Sanofi. JT reports receiving commercial research grants from Merck, Pfizer, Trillium, Hoffmann-LaRoche, Five Prime, Novartis, Incyte, Xencor; is a consultant for Regeneron, Aveo, and Neoleukin. JEG-O reports commercial research grants from Genentech, MedImmune, NanoCarrier, Pfizer, Seagen; and is a consultant for Bayer, Chimerix. S. Ansari, A. Topletz-Erickson, M. W. Schmitt, are employees of and hold ownership interest (including patents) in Seagen. CJ and PZ are former employees and hold ownership interest in Seagen. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- Gruss HJ, Dower SK. Tumor necrosis factor ligand Superfamily: involvement in the pathology of malignant Lymphomas. Blood 1995;85:3378–404. - PubMed
-
- Pellat-Deceunynck C, Bataille R, Robillard N, et al. . Expression of Cd28 and Cd40 in human myeloma cells: a comparative study with normal plasma cells. Blood 1994;84:2597–603. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials