

Predictive value of clinician impression for readmission and postdischarge mortality among neonates and young children in Dar es Salaam, Tanzania and Monrovia, Liberia
- PMID: 37385735
- PMCID: PMC10314694
- DOI: 10.1136/bmjpo-2023-001972
Predictive value of clinician impression for readmission and postdischarge mortality among neonates and young children in Dar es Salaam, Tanzania and Monrovia, Liberia
Abstract
Background: There are no validated clinical decision aids to identify neonates and young children at risk of hospital readmission or postdischarge mortality in sub-Saharan Africa, leaving the decision to discharge a child to a clinician's impression. Our objective was to determine the precision of clinician impression to identify neonates and young children at risk for readmission and postdischarge mortality.
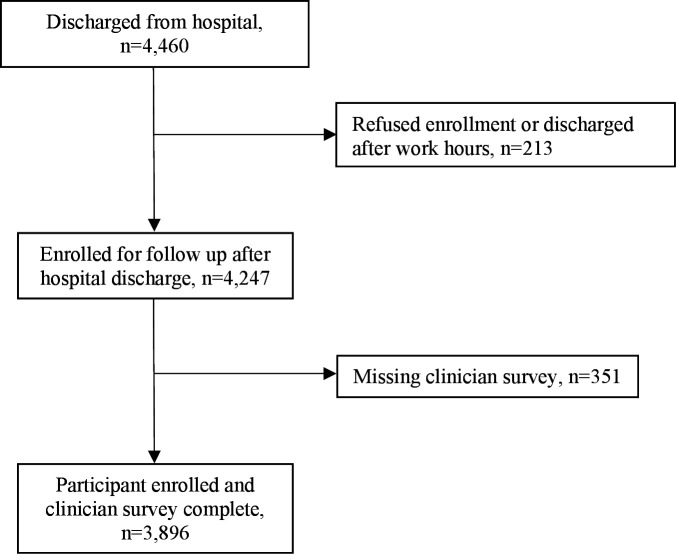
Methods: We conducted a survey study nested in a prospective observational cohort of neonates and children aged 1-59 months followed 60 days after hospital discharge from Muhimbili National Hospital in Dar es Salaam, Tanzania or John F. Kennedy Medical Center in Monrovia, Liberia. Clinicians who discharged each enrolled patient were surveyed to determine their perceived probability of the patient's risk of 60-day hospital readmission or postdischarge mortality. We calculated the area under the precision-recall curve (AUPRC) to determine the precision of clinician impression for both outcomes.
Results: Of 4247 discharged patients, 3896 (91.7%) had available clinician surveys and 3847 (98.7%) had 60-day outcomes available: 187 (4.8%) were readmitted and 120 (3.1%) died within 60 days of hospital discharge. Clinician impression had poor precision in identifying neonates and young children at risk of hospital readmission (AUPRC: 0.06, 95% CI: 0.04 to 0.08) and postdischarge mortality (AUPRC: 0.05, 95% CI: 0.03 to 0.08). Patients for whom clinicians attributed inability to pay for future medical treatment as the reason for risk for unplanned hospital readmission had 4.76 times the odds hospital readmission (95% CI: 1.31 to 17.25, p=0.02).
Conclusions: Given the poor precision of clinician impression alone to identify neonates and young children at risk of hospital readmission and postdischarge mortality, validated clinical decision aids are needed to aid in the identification of young children at risk for these outcomes.
Keywords: health services research; mortality; neonatology.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization . Child mortality (under 5 years). 2022. Available: https://www.who.int/news-room/fact-sheets/detail/levels-and-trends-in-ch... [Accessed May 2023].
-
- Pavlinac PB, Singa BO, Tickell KD, et al. . Azithromycin for the prevention of Rehospitalisation and death among Kenyan children being discharged from hospital: a double-blind, placebo-controlled, randomised controlled trial. Lancet Glob Health 2021;9:e1569–78. 10.1016/S2214-109X(21)00347-8 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources