

External validation of a risk model predicting failure of salvage focal ablation for prostate cancer
- PMID: 37385981
- PMCID: PMC10615865
- DOI: 10.1111/bju.16102
External validation of a risk model predicting failure of salvage focal ablation for prostate cancer
Abstract
Objectives: To externally validate a published model predicting failure within 2 years after salvage focal ablation in men with localised radiorecurrent prostate cancer using a prospective, UK multicentre dataset.
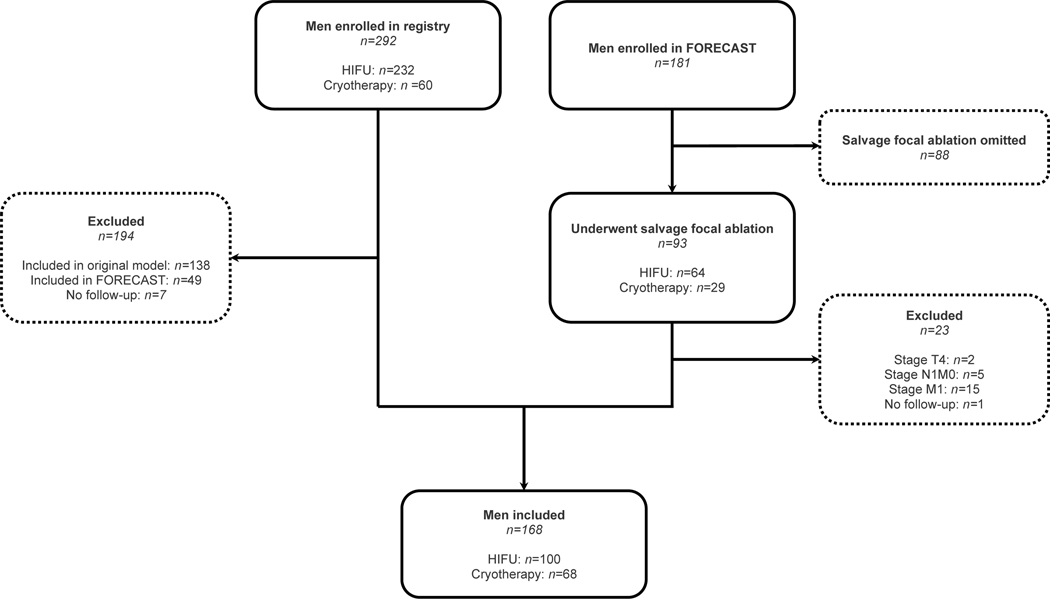
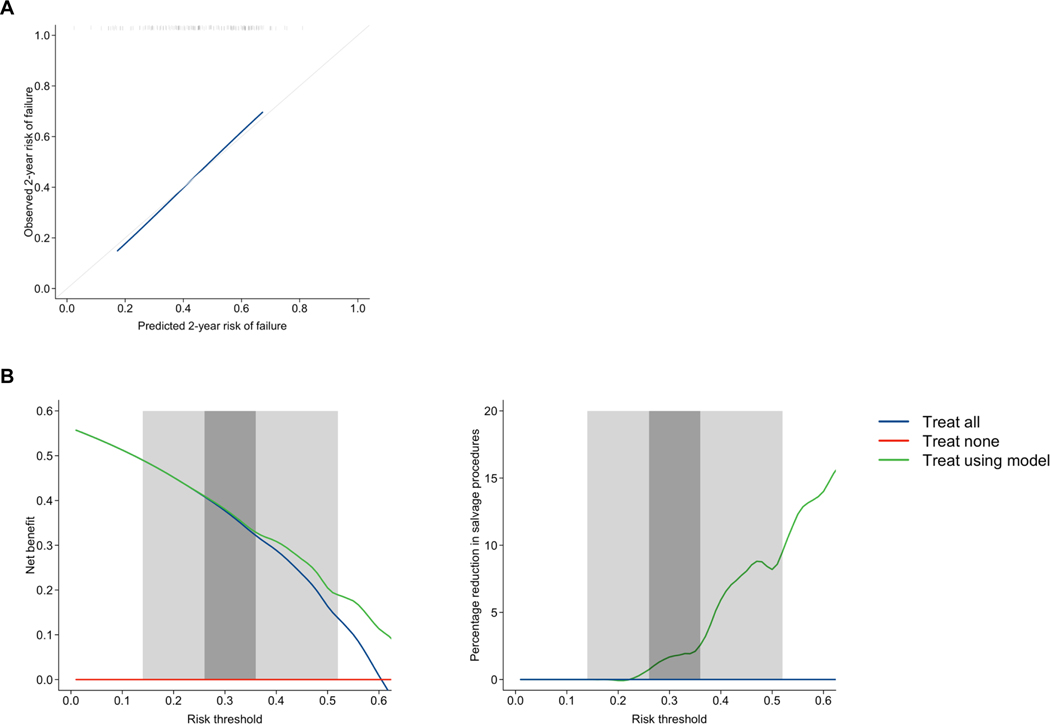
Patients and methods: Patients with biopsy-confirmed ≤T3bN0M0 cancer after previous external beam radiotherapy or brachytherapy were included from the FOcal RECurrent Assessment and Salvage Treatment (FORECAST) trial (NCT01883128; 2014-2018; six centres), and from the high-intensity focussed ultrasound (HIFU) Evaluation and Assessment of Treatment (HEAT) and International Cryotherapy Evaluation (ICE) UK-based registries (2006-2022; nine centres). Eligible patients underwent either salvage focal HIFU or cryotherapy, with the choice based predominantly on anatomical factors. Per the original multivariable Cox regression model, the predicted outcome was a composite failure outcome. Model performance was assessed at 2 years post-salvage with discrimination (concordance index [C-index]), calibration (calibration curve and slope), and decision curve analysis. For the latter, two clinically-reasonable risk threshold ranges of 0.14-0.52 and 0.26-0.36 were considered, corresponding to previously published pooled 2-year recurrence-free survival rates for salvage local treatments.
Results: A total of 168 patients were included, of whom 84/168 (50%) experienced the primary outcome in all follow-ups, and 72/168 (43%) within 2 years. The C-index was 0.65 (95% confidence interval 0.58-0.71). On graphical inspection, there was close agreement between predicted and observed failure. The calibration slope was 1.01. In decision curve analysis, there was incremental net benefit vs a 'treat all' strategy at risk thresholds of ≥0.23. The net benefit was therefore higher across the majority of the 0.14-0.52 risk threshold range, and all of the 0.26-0.36 range.
Conclusion: In external validation using prospective, multicentre data, this model demonstrated modest discrimination but good calibration and clinical utility for predicting failure of salvage focal ablation within 2 years. This model could be reasonably used to improve selection of appropriate treatment candidates for salvage focal ablation, and its use should be considered when discussing salvage options with patients. Further validation in larger, international cohorts with longer follow-up is recommended.
Keywords: ablation; cryotherapy; failure; focal therapy; high-intensity focussed ultrasound; prediction model; prostate cancer; radiotherapy; recurrence; salvage.
© 2023 The Authors. BJU International published by John Wiley & Sons Ltd on behalf of BJU International.
Conflict of interest statement
Conflicts of interest:
The remaining authors have nothing to disclose.
Figures



References
-
- Results of the NPCA Prospective Audit in England and Wales for men diagnosed from 1 National Prostate Cancer Audit 2022.
-
- Ma TM, Chu FI, Sandler H, Feng FY, Efstathiou JA, Jones CU, et al. Local Failure Events in Prostate Cancer Treated with Radiotherapy: A Pooled Analysis of 18 Randomized Trials from the Meta-analysis of Randomized Trials in Cancer of the Prostate Consortium (LEVIATHAN). Eur Urol 2022;82:487–98. 10.1016/J.EURURO.2022.07.011. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
