

Efficacy, safety and pharmacokinetics of Unecritinib (TQ-B3101) for patients with ROS1 positive advanced non-small cell lung cancer: a Phase I/II Trial
- PMID: 37385995
- PMCID: PMC10310851
- DOI: 10.1038/s41392-023-01454-z
Efficacy, safety and pharmacokinetics of Unecritinib (TQ-B3101) for patients with ROS1 positive advanced non-small cell lung cancer: a Phase I/II Trial
Abstract
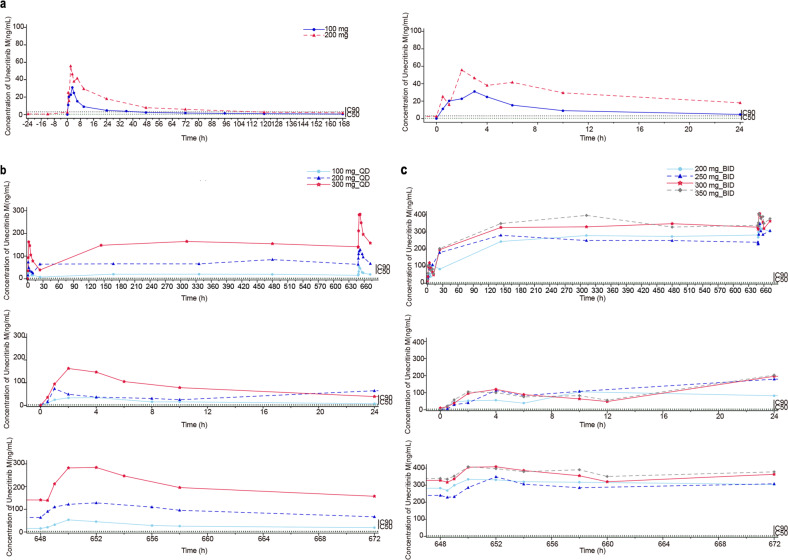
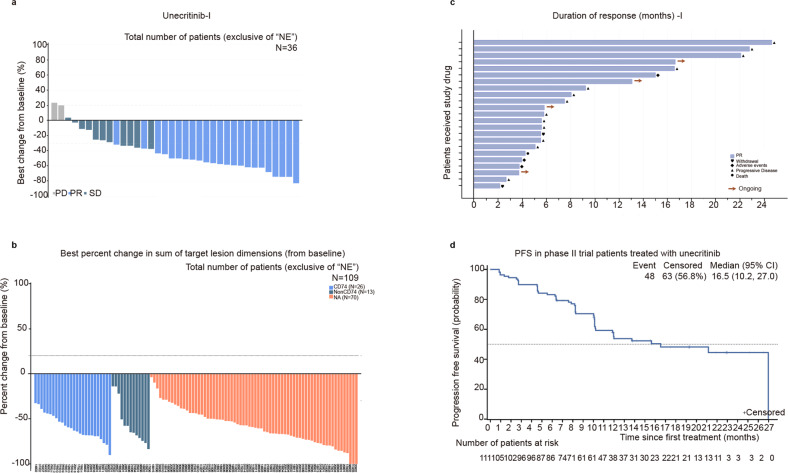
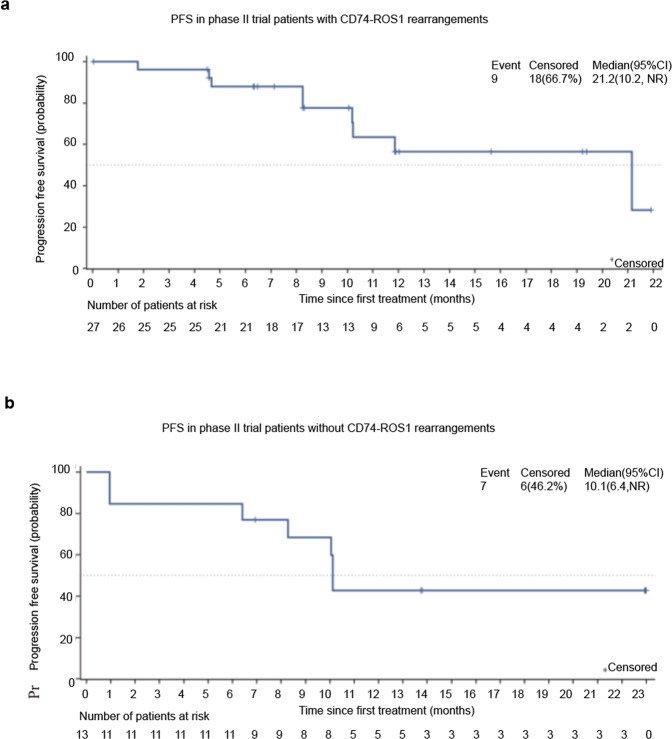
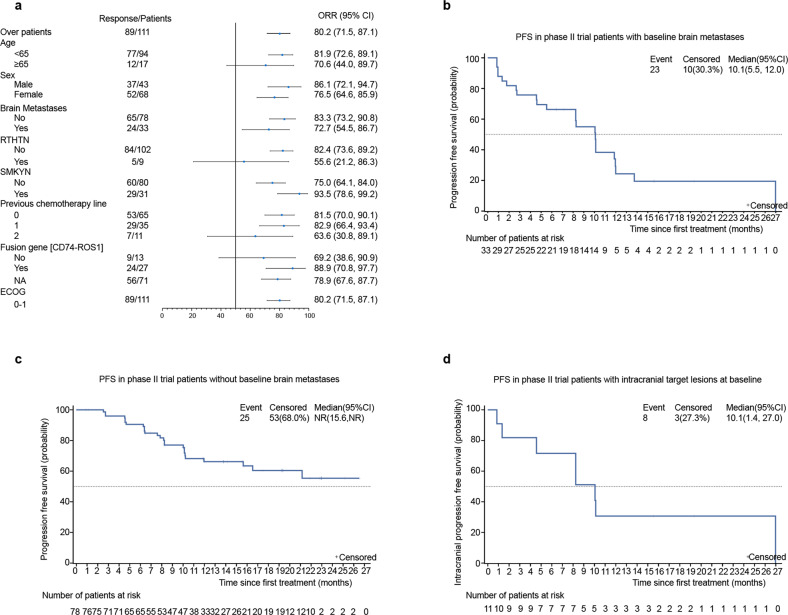
This phase I/II trial characterized the tolerability, safety, and antitumor activities of unecritinib, a novel derivative of crizotinib and a multi-tyrosine kinase inhibitor targeting ROS1, ALK, and c-MET, in advanced tumors and ROS1 inhibitor-naive advanced or metastatic non-small cell lung cancer (NSCLC) harboring ROS1 rearrangements. Eligible patients received unecritinib 100, 200, and 300 mg QD, and 200, 250, 300, and 350 mg BID in a 3 + 3 design during dose escalation and 300 and 350 mg BID during expansion. Phase II trial patients received unecritinib 300 mg BID in continuous 28-day cycles until disease progression or unacceptable toxicity. The primary endpoint was the objective response rate (ORR) per independent review committee (IRC). Key secondary endpoints included intracranial ORR and safety. The ORR of 36 efficacy evaluable patients in the phase I trial was 63.9% (95% CI 46.2%, 79.2%). In the phase II trial, 111 eligible patients in the main study cohort received unecritinib. The ORR per IRC was 80.2% (95% CI 71.5%, 87.1%) and the median progression-free survival (PFS) per IRC was 16.5 months (95% CI 10.2, 27.0). Additionally, 46.9% of the patients who received recommended phase II dose of 300 mg BID experienced grade 3 or higher treatment-related adverse events. Treatment-related ocular disorders and neurotoxicity occurred in 28.1% and 34.4% of patients, respectively, but none was grade 3 or higher. Unecritinib is efficacious and safe for ROS1 inhibitor-naive patients with ROS1-positive advanced NSCLC, particularly patients with brain metastases at baseline, strongly supporting that unecritinib should become one of the standards of care for ROS1-positive NSCLC.ClinicalTrials.gov identifier: NCT03019276 and NCT03972189.
© 2023. The Author(s).
Conflict of interest statement
S.L. has received research support from Astra Zeneca, Hutchison, BMS, Heng Rui, Beigene and Roche, Hansoh, Lilly Suzhou Pharmaceutical Co. Ltd; has received speaker fees from Astra Zeneca, Roche, Hansoh, Hengrui Therapeutics; and is an advisor and consultant of Astra Zeneca, Pfizer, Boehringer Ingelheim, Hutchison MediPharma, ZaiLab, GenomiCare, Yuhan Corporation, Menarini, InventisBio Co. Ltd., Shanghai Fosun Pharmaceutical (Group) Co., Ltd., Simcere Zaiming Pharmaceutical Co., Ltd. and Roche. T.W. and J.Z. are employees of Chia Tai Tianqing Pharmaceutical Group Co., Ltd. All the other authors declare no competing interests.
Figures
Similar articles
-
First-in-human phase I study of TQ-B3139 (CT-711) in advanced non-small cell lung cancer patients with ALK and ROS1 rearrangements.Eur J Cancer. 2022 Sep;173:238-249. doi: 10.1016/j.ejca.2022.06.037. Epub 2022 Aug 5. Eur J Cancer. 2022. PMID: 35940055 Clinical Trial.
-
Lorlatinib in non-small-cell lung cancer with ALK or ROS1 rearrangement: an international, multicentre, open-label, single-arm first-in-man phase 1 trial.Lancet Oncol. 2017 Dec;18(12):1590-1599. doi: 10.1016/S1470-2045(17)30680-0. Epub 2017 Oct 23. Lancet Oncol. 2017. PMID: 29074098 Free PMC article. Clinical Trial.
-
Safety and Efficacy of Crizotinib in Patients With Advanced or Metastatic ROS1-Rearranged Lung Cancer (EUCROSS): A European Phase II Clinical Trial.J Thorac Oncol. 2019 Jul;14(7):1266-1276. doi: 10.1016/j.jtho.2019.03.020. Epub 2019 Apr 9. J Thorac Oncol. 2019. PMID: 30978502 Clinical Trial.
-
Efficacy and Safety of Crizotinib in the Treatment of Advanced Non-Small-Cell Lung Cancer with ROS1 Rearrangement or MET Alteration: A Systematic Review and Meta-Analysis.Target Oncol. 2020 Oct;15(5):589-598. doi: 10.1007/s11523-020-00745-7. Target Oncol. 2020. PMID: 32865687
-
Targeted therapies in non-small cell lung cancer: a focus on ALK/ROS1 tyrosine kinase inhibitors.Expert Rev Anticancer Ther. 2018 Jan;18(1):71-80. doi: 10.1080/14737140.2018.1412260. Epub 2017 Dec 6. Expert Rev Anticancer Ther. 2018. PMID: 29187012 Review.
Cited by
-
Updates to the 2024 CSCO advanced non-small cell lung cancer guidelines.Cancer Biol Med. 2025 Feb 24;22(2):77-82. doi: 10.20892/j.issn.2095-3941.2024.0497. Cancer Biol Med. 2025. PMID: 39995197 Free PMC article. No abstract available.
-
Advances in molecular pathology and therapy of non-small cell lung cancer.Signal Transduct Target Ther. 2025 Jun 15;10(1):186. doi: 10.1038/s41392-025-02243-6. Signal Transduct Target Ther. 2025. PMID: 40517166 Free PMC article. Review.
-
Visceral crisis in a patient with non-small cell lung cancer and ROS1::SDC4 fusion: intrinsic resistance to entrectinib via L2026M mutation-a case report.Transl Lung Cancer Res. 2025 May 30;14(5):1862-1869. doi: 10.21037/tlcr-2024-1149. Epub 2025 May 28. Transl Lung Cancer Res. 2025. PMID: 40535089 Free PMC article.
-
[Clinical Practice Guidelines for the Management of Brain Metastases from Non-small Cell Lung Cancer with Actionable Gene Alterations in China (2025 Edition)].Zhongguo Fei Ai Za Zhi. 2025 Jan 20;28(1):1-21. doi: 10.3779/j.issn.1009-3419.2024.102.42. Epub 2025 Jan 7. Zhongguo Fei Ai Za Zhi. 2025. PMID: 39763097 Free PMC article. Chinese.
-
Advances and future directions in ROS1 fusion-positive lung cancer.Oncologist. 2024 Nov 4;29(11):943-956. doi: 10.1093/oncolo/oyae205. Oncologist. 2024. PMID: 39177972 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
