

A single centre prospective study of three device-assisted therapies for Parkinson's disease
- PMID: 37386050
- PMCID: PMC10310730
- DOI: 10.1038/s41531-023-00525-w
A single centre prospective study of three device-assisted therapies for Parkinson's disease
Abstract
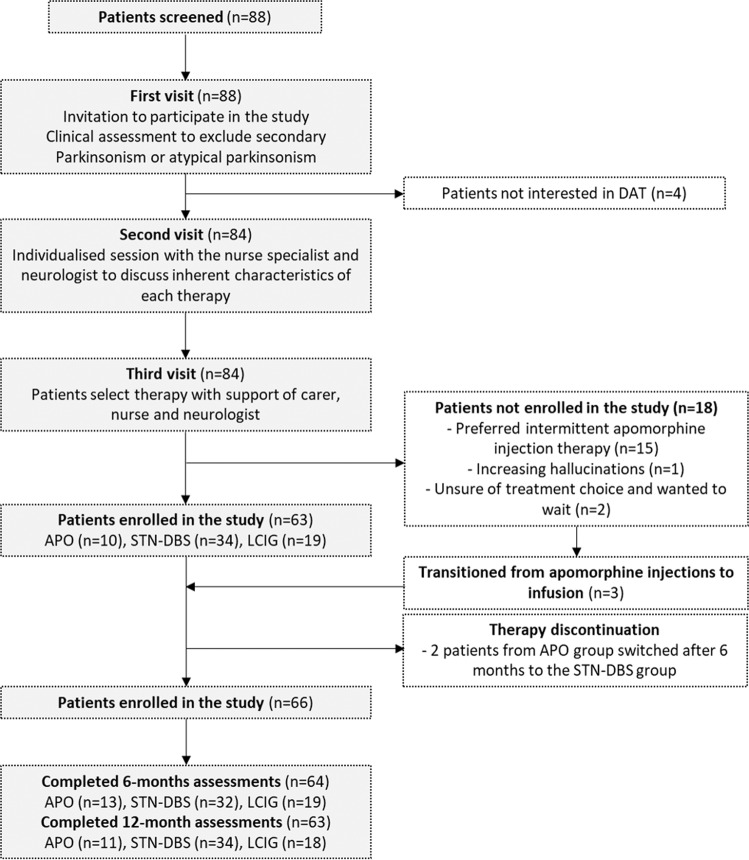
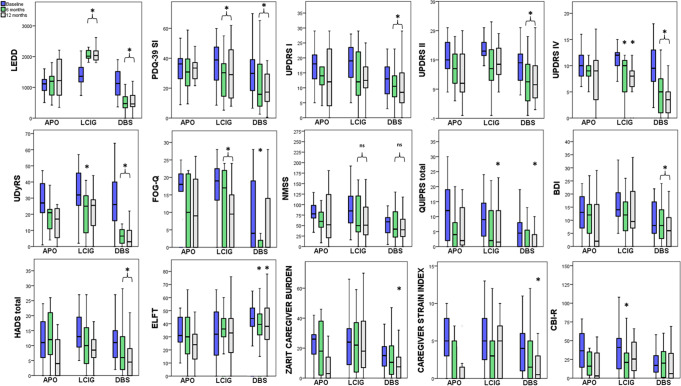
Comparative studies assessing outcomes with the three device-assisted therapies could help to individualise treatment for patients living with Parkinson's disease. We designed a single-centre non-randomised prospective observational study assessing the quality of life (QoL), motor and non-motor outcomes at 6 and 12-months in patients treated with subcutaneous apomorphine continuous 16-hours infusion (APO), levodopa-carbidopa intestinal gel (LCIG) or subthalamic nucleus deep brain stimulation (STN-DBS). In this study, 66 patients were included (13 APO; 19 LCIG; 34 STN-DBS). At baseline, cognitive, non-motor and motor scores were significantly less severe in the STN-DBS group, whereas the LCIG group had a longer disease duration and higher non-motor scores. In the APO group, there were no statistically significant changes in non-motor, motor and QoL scales. The LCIG group had significant changes in QoL and motor scales that were significant after multiple comparison analysis at 6 and 12-months. The STN-DBS group showed improvement in QoL scores and non-motor and motor scores at 6 and 12-months after multiple comparison analysis. In this real-life prospective study, device-assisted therapies showed differences in their effects on QoL and motor and non-motor function at 12-months. However, there were also differences in baseline characteristics of the patient groups that were not based on pre-determined selection criteria. Differences in characteristics of patients offered and/or treatment with different device-assisted therapies may reflect within-centre biases that may, in turn, influence perceptions of treatment efficacy or outcomes. Treatment centres should be aware of this potential confounder when assessing and offering device-assisted treatment options to their patients and potential baseline differences need to be taken into consideration when comparing the results of non-randomised studies.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing non-financial interests but the following competing financial interests: Hugo Morales’s position was funded by an unrestricted donation (the Baffsky Parkinson’s Disease Research Fund) and administered by the Western Sydney Local Health District. Han-Lin Chiang and Yicheng Tai have no financial disclosures. Neil Mahant, Ainhi Ha, Florence Chang, David Tsui and Samuel Kim receive salary from NSW Health. Jane Griffith and Donna Galea nursing salaries are partly funded by unrestricted grants to the Western Sydney Local Health District from Abbvie. Victor Fung receives a salary from NSW Health, has received research grants from the National Health and Medical Research Council of Australia, and is on advisory boards and/or has received travel grants from Abbott/AbbVie, Allergan, Boehringer-Ingelheim, Hospira, Ipsen, Lundbeck, Novartis, Parkinson’s KinetiGraph, Solvay, and UCB. The remaining authors declare no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
