

Navigated, percutaneous, three-step technique for lumbar and sacral screw placement: a novel, minimally invasive, and maximally safe strategy
- PMID: 37386233
- PMCID: PMC10310656
- DOI: 10.1186/s10195-023-00696-5
Navigated, percutaneous, three-step technique for lumbar and sacral screw placement: a novel, minimally invasive, and maximally safe strategy
Abstract
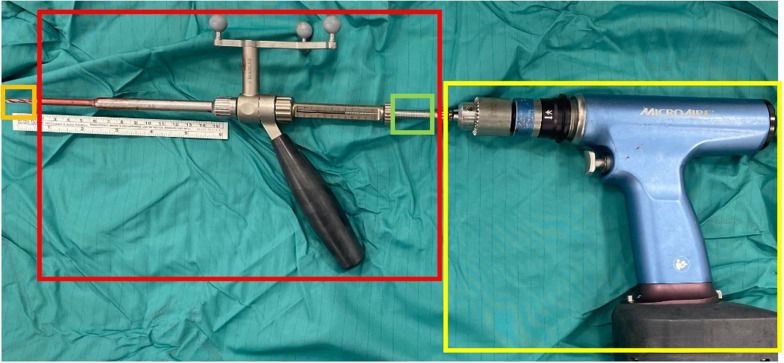
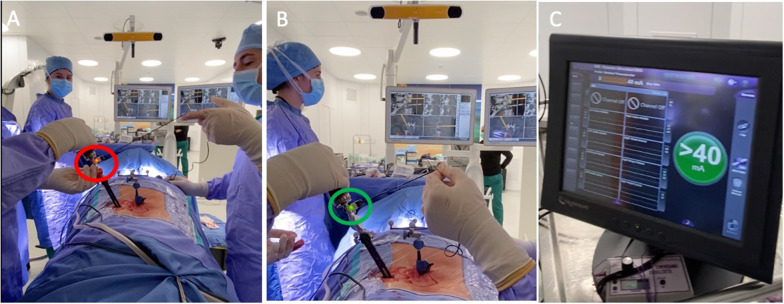
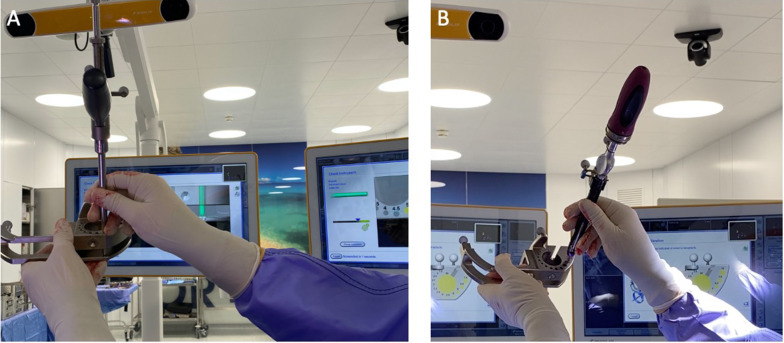
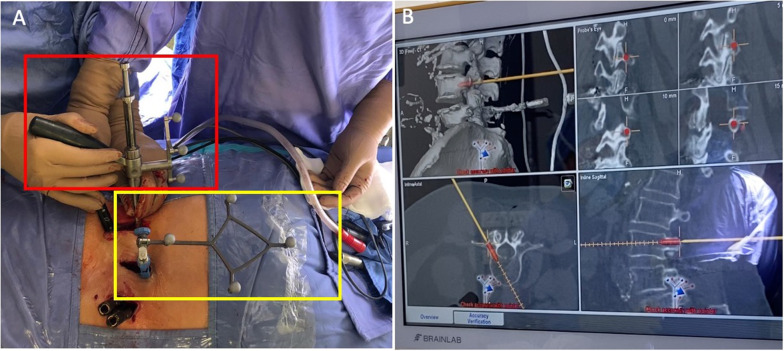
Background: Minimally invasive spine surgery is a field of active and intense research. Image-guided percutaneous pedicle screw (PPS) placement is a valid alternative to the standard free-hand technique, thanks to technological advancements that provide potential improvement in accuracy and safety. Herein, we describe the clinical results of a surgical technique exploiting integration of neuronavigation and intraoperative neurophysiological monitoring (IONM) for minimally invasive PPS.
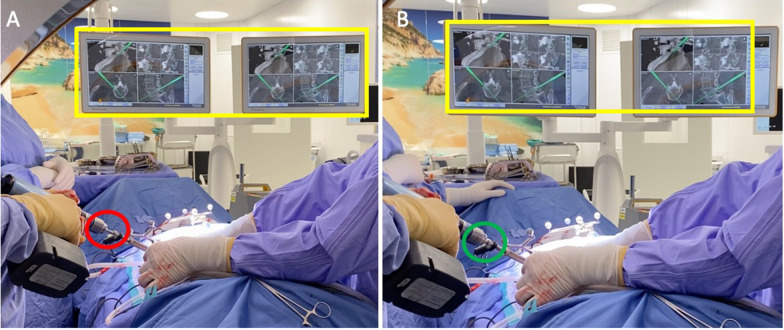
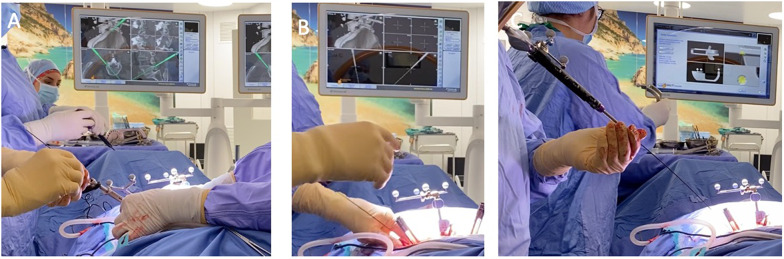
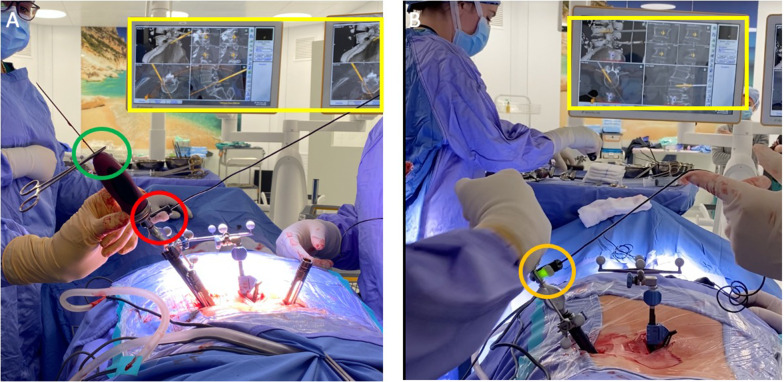
Materials and methods: An intraoperative-computed tomography (CT)-based neuronavigation system was combined with IONM in a three-step technique for PPS. Clinical and radiological data were collected to evaluate the safety and efficacy of the procedure. The accuracy of PPS placement was classified according to the Gertzbein-Robbins scale.
Results: A total of 230 screws were placed in 49 patients. Only two screws were misplaced (0.8%); nevertheless, no clinical sign of radiculopathy was experienced by these patients. The majority of the screws (221, 96.1%) were classified as grade A according to Gertzbein-Robbins scale, seven screws were classified as grade B, one screw was classified as grade D, and one last screw was classified as grade E.
Conclusions: The proposed three-step, navigated, percutaneous procedure offers a safe and accurate alternative to traditional techniques for lumbar and sacral pedicle screw placement. Level of Evidence Level 3. Trial registration Not applicable.
Keywords: Lumbo–sacral instrumentation; Minimally invasive spine surgery; Navigated drill guide; Percutaneous navigated screw placement.
© 2023. The Author(s).
Conflict of interest statement
The authors declare they have no competing financial interests with the current study.
Figures
References
-
- Costa F, Tosi G, Attuati L, Cardia A, Ortolina A, Grimaldi M, Galbusera F, Fornari M. Radiation exposure in spine surgery using an image-guided system based on intraoperative cone-beam computed tomography: analysis of 107 consecutive cases. SPI. 2016;25(5):654–659. doi: 10.3171/2016.3.SPINE151139. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
