

Barriers to delirium screening and management during hospital admission: a qualitative analysis of inpatient nursing perspectives
- PMID: 37386400
- PMCID: PMC10311863
- DOI: 10.1186/s12913-023-09681-4
Barriers to delirium screening and management during hospital admission: a qualitative analysis of inpatient nursing perspectives
Abstract
Background: Delirium in hospitalized patients is a major public health issue, yet delirium is often unrecognized and missed during inpatient admission. The objective of this study was to identify barriers to delirium screening, identification, and management from a nursing perspective on inpatient, acute care units.
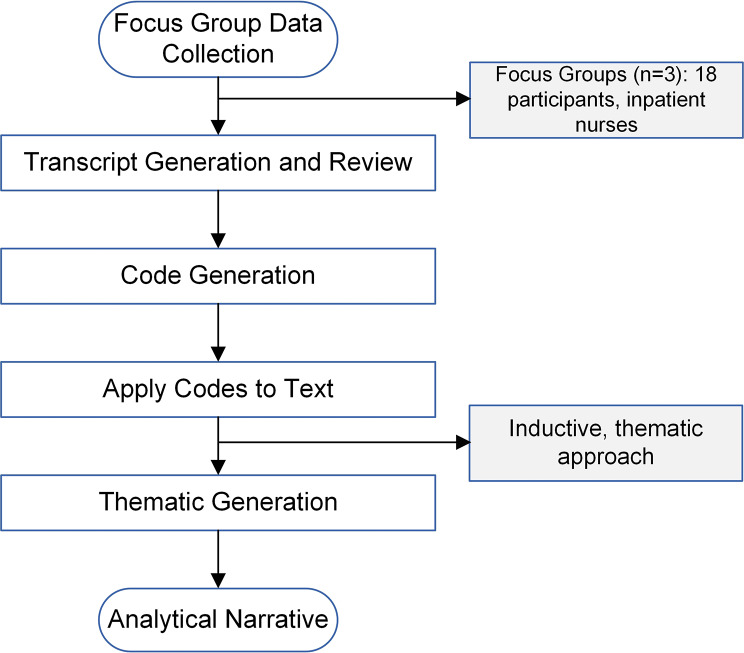
Methods: This was a pre-implementation, diagnostic evaluation study to determine current practice patterns and potential barriers to optimizing delirium care at a major university hospital. A qualitative approach was used, which included focus groups of inpatient nurses working on major medical and surgical acute care units. Focus groups were conducted until signs of thematic saturation were present, and data were analyzed via inductive thematic analysis, without predetermined theories or structures. A consensus approach was utilized for transcript coding, and final themes were generated after multiple reviews of initial themes against transcript datasets.
Results: Focus group sessions (n = 3) were held with 18 nurses across two major inpatient units. Nurses reported several barriers to successful delirium screening and management. Specific challenges included difficulty with using delirium screening tools, an organizational culture not conducive to delirium prevention, and competing clinical priorities. Proposed solutions were also discussed, including decision-support systems with automated pager alerts and associated delirium order sets, which may help improve delirium care coordination and standardization.
Conclusion: At a major university hospital, nurses affirm the difficulty experienced with delirium screening and identification, particularly due to screening tool challenges, cultural barriers, and clinical workload. These impediments may serve as targets for a future implementation trial to improve delirium screening and management.
Keywords: Decision support (clinical); Evaluation methodology; Implementation science; Quality Improvement.
© 2023. The Author(s).
Conflict of interest statement
Ms. McKinney, Dr. Shah, Dr. Min, an Dr. Vlisides receive support from Blue Cross Blue Shield of Michigan (Detroit, Michigan, USA) for quality improvement work related to delirium. The opinions, beliefs, and viewpoints expressed by the authors do not necessarily reflect the opinions, beliefs, and viewpoints of Blue Cross Blue Shield of Michigan/Blue Care Network or any of its employees. Dr. Ragheb, Dr. Norcott, and Ms. Benn have no conflicts of interest to report.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
