

Attention-deficit/hyperactivity disorder (ADHD) symptoms and their relation to diagnosed ADHD, sociodemographic characteristics, and substance use among patients receiving opioid agonist therapy: a Norwegian cohort study
- PMID: 37386438
- PMCID: PMC10308780
- DOI: 10.1186/s12888-023-04980-w
Attention-deficit/hyperactivity disorder (ADHD) symptoms and their relation to diagnosed ADHD, sociodemographic characteristics, and substance use among patients receiving opioid agonist therapy: a Norwegian cohort study
Abstract
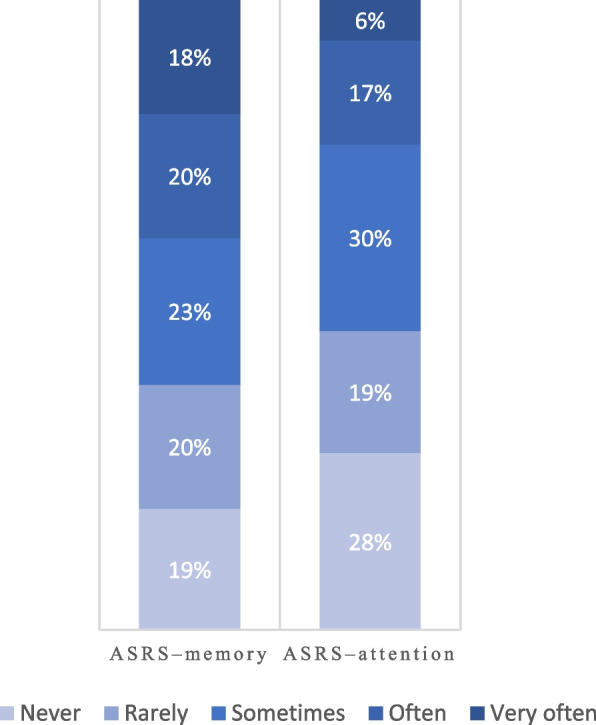
Background: Attention-deficit/hyperactivity disorder (ADHD) symptoms may challenge sufficient treatment of substance use and mental disorders. The literature on the extent of such symptoms among patients receiving opioid agonist therapy (OAT) is scarce. This study examined ADHD symptoms using the ADHD self-report scale (ASRS) and the association between the 'ASRS-memory' and 'ASRS-attention' scores and substance use and sociodemographic characteristics among patients receiving OAT.
Methods: We used data from assessment visits of a cohort of patients in Norway. In total, 701 patients were included from May 2017 to March 2022. All patients responded at least once to two ASRS questions assessing memory and attention, respectively. Ordinal regression analyses were performed to investigate whether the two obtained scores were associated with age, sex, frequent substance use, injecting use, housing status, and educational attainment at baseline, i.e., the first assessment, and over time. The results are presented as odds ratios (OR) with 95% confidence intervals (CI). Additionally, a subsample of 225 patients completed an extended interview, including the ASRS-screener and collection of registered mental disorder diagnoses from the medical records. Standard cutoffs were used to define the presence of each ASRS symptom or a positive ASRS-screener ('ASRS-positive').
Results: At baseline, 428 (61%) and 307 (53%) patients scored over the cutoffs on the 'ASRS-memory' and 'ASRS-attention,' respectively. Frequent cannabis use was associated with higher 'ASRS-memory' (OR: 1.7, 95% CI: 1.1-2.6) and 'ASRS-attention' (1.7, 1.1-2.5) scores compared with less or no use at baseline, though reduced score on the 'ASRS-memory' over time (0.7, 0.6-1.0). At baseline, frequent stimulant use (1.8, 1.0-3.2) and low educational attainment (0.1, 0.0-0.8) were associated with higher 'ASRS-memory' scores. In the subsample fulfilling the ASRS-screener, 45% of the patients were 'ASRS-positive,' of whom 13% with a registered ADHD diagnosis.
Conclusions: Our findings illustrate a relationship between the ASRS-memory and -attention scores and frequent cannabis and stimulant use. Furthermore, nearly half of the subsample was 'ASRS-positive.' Patients receiving OAT might benefit from being further assessed for ADHD, but improved diagnostic methods are required.
Keywords: Adult ADHD self-report scale; Attention-deficit/hyperactivity disorder symptoms; Injecting substance use; Opioid substitution treatment; Substance-related disorders.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Diagnostic and statistical manual of mental disorders : DSM-5. Arlington, VA: American Psychiatric Association; 2013.
-
- van de Glind G, Konstenius M, Koeter MWJ, van Emmerik-van OK, Carpentier PJ, Kaye S, Degenhardt L, Skutle A, Franck J, Bu ET, et al. Variability in the prevalence of adult ADHD in treatment seeking substance use disorder patients: results from an international multi-center study exploring DSM-IV and DSM-5 criteria. Drug Alcohol Depend. 2014;134:158–166. doi: 10.1016/j.drugalcdep.2013.09.026. - DOI - PMC - PubMed
-
- Wilens TE. Impact of ADHD and its treatment on substance abuse in adults. J Clin Psychiatry. 2004;65(Suppl 3):38–45. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
