

Association between non-insulin-based insulin resistance indices and cardiovascular events in patients undergoing percutaneous coronary intervention: a retrospective study
- PMID: 37386494
- PMCID: PMC10311786
- DOI: 10.1186/s12933-023-01898-1
Association between non-insulin-based insulin resistance indices and cardiovascular events in patients undergoing percutaneous coronary intervention: a retrospective study
Abstract
Background: Insulin resistance (IR) has been confirmed that getting involved in the pathophysiological process of cardiovascular diseases (CVD). Recently, increasing evidence suggests metabolic score for insulin resistance (METS-IR), triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) ratio, triglyceride and glucose (TyG) index, triglyceride glucose-body mass (TyG-BMI) index are simple and reliable surrogates for IR. However, their abilities in predicting cardiovascular outcomes in patients undergoing percutaneous coronary intervention (PCI) are not well explored. Therefore, this study aimed to investigate the association and evaluate the predictive performance of each index.
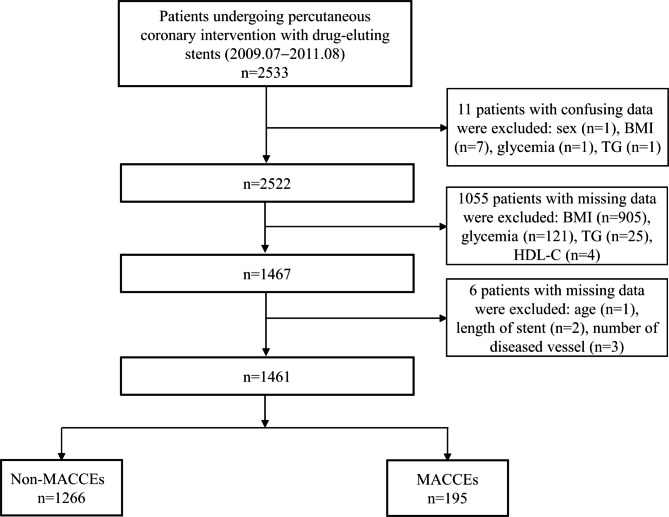
Methods: A total of 2533 consecutive participants undergoing PCI were included in this study, and the data from 1461 patients were used to determine the correlation of these non-insulin-based IR indices with major adverse cardiac and cerebrovascular events (MACCEs) via performing the multivariate logistic models and restricted cubic splines (RCS).
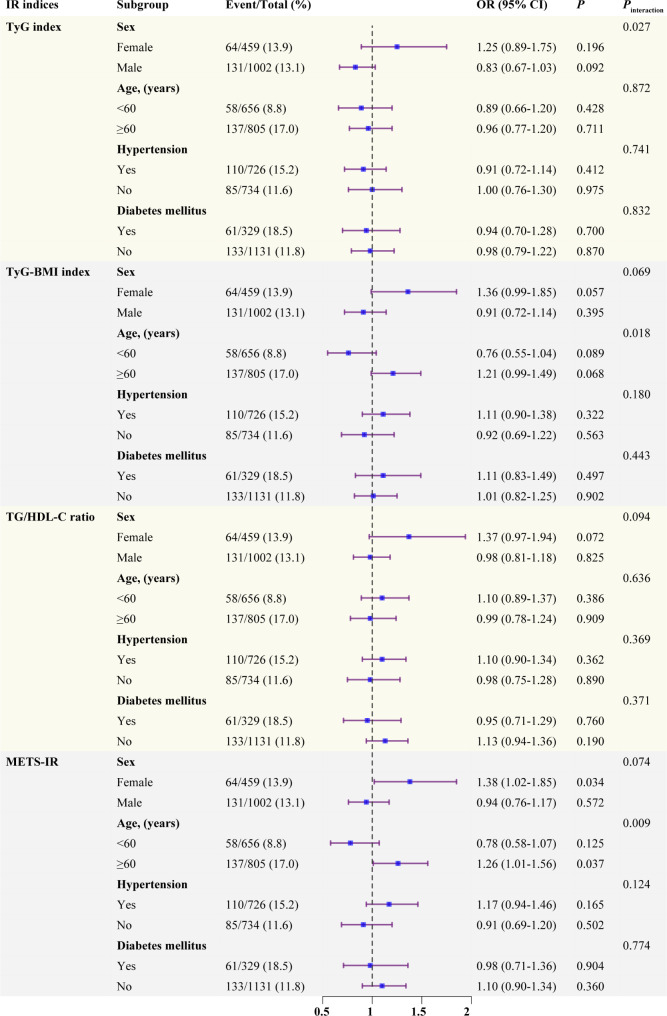
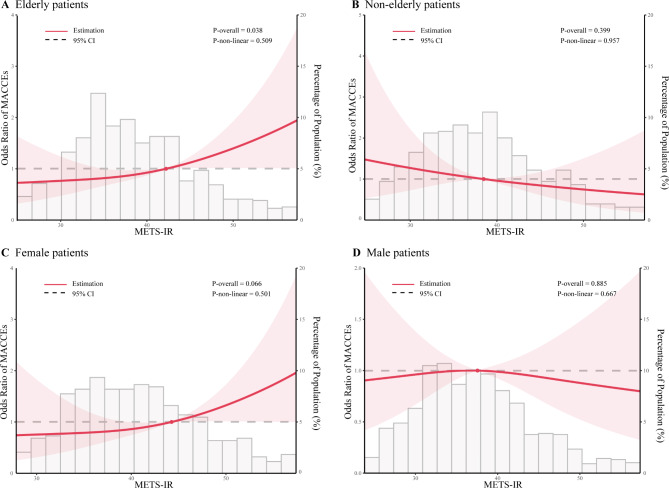
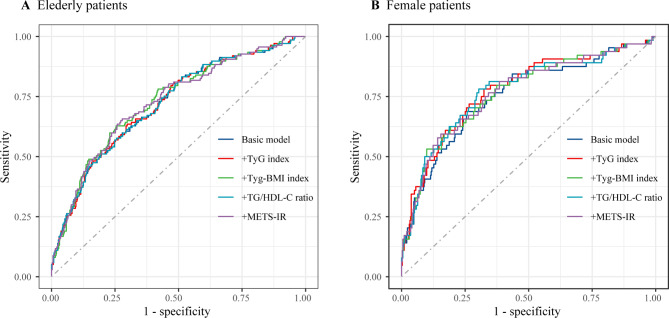
Results: During a median of 29.8 months follow-up, 195 cases of 1461 patients experienced incident MACCEs. In the overall population, both univariate and multivariate logistic regression analyses indicated no statistically significant connection between these IR indices and MACCEs. Subgroup analyses revealed significant interactions between age subgroups and TyG-BMI index, as well as METS-IR, and between sex subgroups and TyG index. In elderly patients, per 1.0-SD increment in TyG-BMI index and METS-IR had a significant association with MACCEs, with odds ratios (ORs) [95% confidence interval (CI)] of 1.24 (1.02-1.50) and 1.27 (1.04-1.56), respectively (both P < 0.05). Moreover, in female patients, all the IR indices showed significant associations with MACCEs. Multivariable-adjusted RCS curves demonstrated a linear relationship between METS-IR and MACCEs in elderly and female patients, respectively. However, all the IR indices failed to enhance the predictive performance of the basic risk model for MACCEs.
Conclusion: All the four IR indices showed a significant association with MACCEs in female individuals, whereas only TyG-BMI index and METS-IR showed associations in elderly patients. Although the inclusion of these IR indices did not improve the predictive power of basic risk model in either female or elderly patients, METS-IR appears to be the most promising index for secondary prevention of MACCEs and risk stratification in patients undergoing PCI.
Keywords: Cardiovascular outcomes; Coronary artery disease; Insulin resistance; Metabolic score for insulin resistance; Percutaneous coronary intervention.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Neumann F-J, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019, 40(2). - PubMed
-
- Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022, 79(2). - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Miscellaneous
