

Selective spinal anesthesia with hyperbaric prilocaine provides better perioperative pain control than local anesthesia for ambulatory inguinal hernia repair without affecting discharging time: a randomized controlled trial
- PMID: 37386519
- PMCID: PMC10245599
- DOI: 10.1186/s44158-022-00034-x
Selective spinal anesthesia with hyperbaric prilocaine provides better perioperative pain control than local anesthesia for ambulatory inguinal hernia repair without affecting discharging time: a randomized controlled trial
Abstract
Purpose: Local anesthesia is the most used anesthetic technique for inguinal hernia repair, despite its unpredictability. Selective spinal anesthesia with a short-term local anesthetic guarantees rapid recovery, predictable duration and low incidence of side effects. We tried to assess the efficacy of this neuraxial technique in ambulatory setting.
Methods: One hundred thirty-two ASA I-III, aged > 18 patients scheduled for inguinal hernia repair have been randomized into two groups receiving unilateral spinal anesthesia with 40 mg of hyperbaric prilocaine (group A) or local anesthesia with mepivacaine (group B).
Primary endpoint: intraoperative and post-operative NRS. Other outcomes: sensory block onset, need for opiates and deep sedation, surgery duration, and time to discharge.
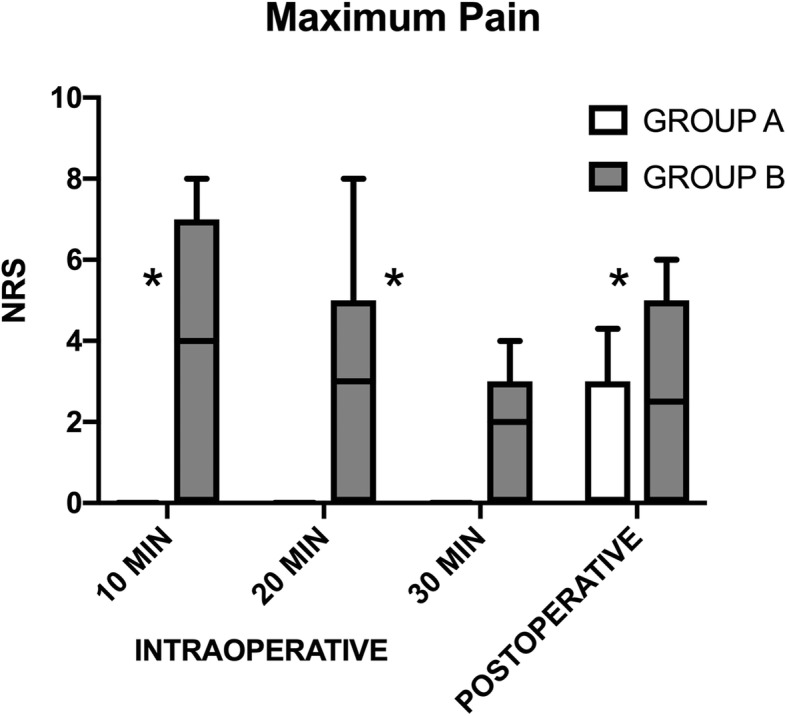
Results: Group A: intraoperative NRS was 0 in 100% of patients; post-operative maximum NRS was > 3 in 12.12% of patients. Group B: mean intraoperative NRS was 4; mean post-operative NRS was 2.5. Spinal anesthesia resulted superior in controlling both intraoperative and post-operative pain (p < 0.00001; p = 0.008). Mean time of the motor block resolution in group A was 98 ± 2 min. Mean time to discharge was not significantly different between groups. Surgical time was significantly different between the two groups (mean time of 37 ± 3.2 min group A; 54 ± 6 min group B-p < 0.00001).
Conclusion: Spinal anesthesia group patients had significantly less pain than local anesthesia group, both intraoperatively and post-operatively, without differences in time to discharge, incidence of complications and with improvement of surgical time. More randomized controlled trials are needed to confirm this hypothesis.
Trial registration: NCT05136534 . Registered November 29, 2021-Retrospectively registered.
Keywords: Ambulatory surgery; Hyperbaric prilocaine; Inguinal hernia repair; Regional anesthesia; Spinal anesthesia.
© 2022. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests.
Figures

References
-
- Jenkins JT, O'Dwyer PJ. Inguinal hernias. Bmj. 2008;336(7638):269–272. doi: 10.1136/bmj.39450.428275.AD. - DOI - PMC - PubMed
-
- Jacquet E, Puche P, Alahyane J, Jaber S, Carabalona JP, Bessaou D, et al. Evaluation of inguinal hernia in ambulatory surgery: a prospective monocentric study on 1009 inguinal hernia. Ambul Surg. 2006;12(4):167–171. doi: 10.1016/j.ambsur.2005.11.002. - DOI
Associated data
LinkOut - more resources
Full Text Sources