

Machine learning in perioperative medicine: a systematic review
- PMID: 37386544
- PMCID: PMC8761048
- DOI: 10.1186/s44158-022-00033-y
Machine learning in perioperative medicine: a systematic review
Abstract
Background: Risk stratification plays a central role in anesthetic evaluation. The use of Big Data and machine learning (ML) offers considerable advantages for collection and evaluation of large amounts of complex health-care data. We conducted a systematic review to understand the role of ML in the development of predictive post-surgical outcome models and risk stratification.
Methods: Following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, we selected the period of the research for studies from 1 January 2015 up to 30 March 2021. A systematic search in Scopus, CINAHL, the Cochrane Library, PubMed, and MeSH databases was performed; the strings of research included different combinations of keywords: "risk prediction," "surgery," "machine learning," "intensive care unit (ICU)," and "anesthesia" "perioperative." We identified 36 eligible studies. This study evaluates the quality of reporting of prediction models using the Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) checklist.
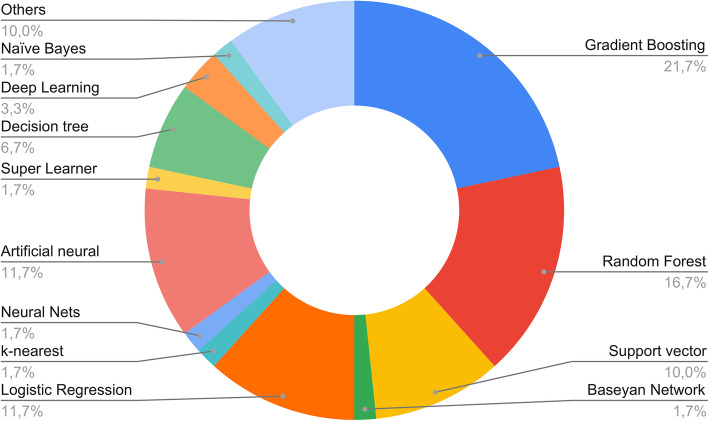
Results: The most considered outcomes were mortality risk, systemic complications (pulmonary, cardiovascular, acute kidney injury (AKI), etc.), ICU admission, anesthesiologic risk and prolonged length of hospital stay. Not all the study completely followed the TRIPOD checklist, but the quality was overall acceptable with 75% of studies (Rev #2, comm #minor issue) showing an adherence rate to TRIPOD more than 60%. The most frequently used algorithms were gradient boosting (n = 13), random forest (n = 10), logistic regression (LR; n = 7), artificial neural networks (ANNs; n = 6), and support vector machines (SVM; n = 6). Models with best performance were random forest and gradient boosting, with AUC > 0.90.
Conclusions: The application of ML in medicine appears to have a great potential. From our analysis, depending on the input features considered and on the specific prediction task, ML algorithms seem effective in outcomes prediction more accurately than validated prognostic scores and traditional statistics. Thus, our review encourages the healthcare domain and artificial intelligence (AI) developers to adopt an interdisciplinary and systemic approach to evaluate the overall impact of AI on perioperative risk assessment and on further health care settings as well.
Keywords: Anesthesia; ICU; Machine learning; Perioperative; Risk prediction; Surgery.
© 2022. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests.
Figures





References
-
- Bose S, Talmor D. (2018) Who is a high-risk surgical patient? Curr Opin Crit Care;24(6):547-553. doi: 10.1097/MCC.0000000000000556. PMID: 30308542. - PubMed
-
- Rajkomar A, Dean J, Kohane I. (2019) Machine Learning in Medicine. N Engl J Med. 380(14):1347-1358. doi: 10.1056/NEJMra1814259. PMID: 30943338. - PubMed
-
- Nashef SA, Roques F, Michel P, Gauducheau E, Lemeshow S, Salamon R. (1999). European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg. 16(1):9-13. doi: 10.1016/s1010-7940(99)00134-7. PMID: 10456395. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources