

Organ dysfunction, injury, and failure in cardiogenic shock
- PMID: 37386552
- PMCID: PMC10308671
- DOI: 10.1186/s40560-023-00676-1
Organ dysfunction, injury, and failure in cardiogenic shock
Abstract
Background: Cardiogenic shock (CS) is caused by primary cardiac dysfunction and induced by various and heterogeneous diseases (e.g., acute impairment of cardiac performance, or acute or chronic impairment of cardiac performance).
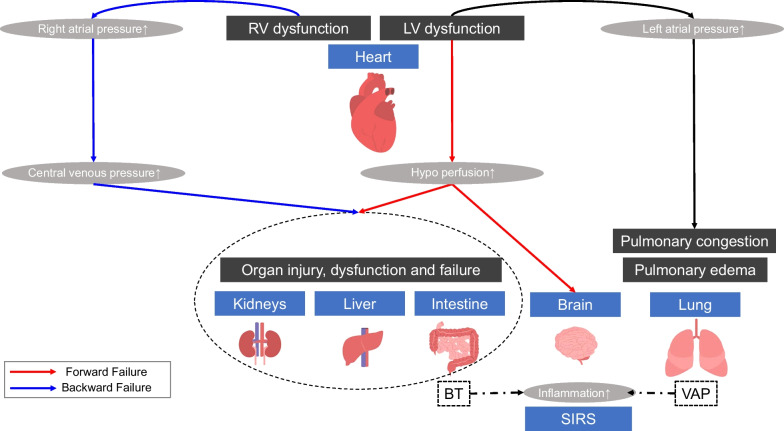
Main body: Although a low cardiac index is a common finding in patients with CS, the ventricular preload, pulmonary capillary wedge pressure, central venous pressure, and systemic vascular resistance might vary between patients. Organ dysfunction has traditionally been attributed to the hypoperfusion of the organ due to either progressive impairment of the cardiac output or intravascular volume depletion secondary to CS. However, research attention has recently shifted from this cardiac output ("forward failure") to venous congestion ("backward failure") as the most important hemodynamic determinant. Both hypoperfusion and/or venous congestion by CS could lead to injury, impairment, and failure of target organs (i.e., heart, lungs, kidney, liver, intestines, brain); these effects are associated with an increased mortality rate. Treatment strategies for the prevention, reduction, and reversal of organ injury are warranted to improve morbidity in these patients. The present review summarizes recent data regarding organ dysfunction, injury, and failure.
Conclusions: Early identification and treatment of organ dysfunction, along with hemodynamic stabilization, are key components of the management of patients with CS.
Keywords: Acute decompensated heart failure; Biomarker; Inflammation; Mortality.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Freis ED, Schnaper HW, Johnson RL, Schreiner GE. Hemodynamic alterations in acute myocardial infarction. I. Cardiac output, mean arterial pressure, total peripheral resistance, central and total blood volumes, venous pressure and average circulation time. J Clin Invest. 1952;31:131–140. doi: 10.1172/JCI102584. - DOI - PMC - PubMed
-
- Vallabhajosyula S, Dewaswala N, Sundaragiri PR, Bhopalwala HM, Cheungpasitporn W, Doshi R, et al. Cardiogenic shock complicating ST-segment elevation myocardial infarction: an 18-year analysis of temporal trends, epidemiology, management, and outcomes. Shock. 2022;57:360–369. doi: 10.1097/SHK.0000000000001895. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
