

Epidemiology of ventilator-associated pneumonia in ICU COVID-19 patients: an alarming high rate of multidrug-resistant bacteria
- PMID: 37386603
- PMCID: PMC9389502
- DOI: 10.1186/s44158-022-00065-4
Epidemiology of ventilator-associated pneumonia in ICU COVID-19 patients: an alarming high rate of multidrug-resistant bacteria
Abstract
Background: COVID‑19 is a novel cause of acute respiratory distress syndrome (ARDS) that leads patients to intensive care unit (ICU) admission requiring invasive ventilation, who consequently are at risk of developing of ventilator‑associated pneumonia (VAP). The aim of this study was to assess the incidence, antimicrobial resistance, risk factors, and outcome of VAP in ICU COVID-19 patients in invasive mechanical ventilation (MV).
Methods: Observational prospective study including adult ICU admissions between January 1, 2021, and June 31, 2021, with confirmed COVID-19 diagnosis were recorded daily, including demographics, medical history, ICU clinical data, etiology of VAPs, and the outcome. The diagnosis of VAP was based on multi-criteria decision analysis which included a combination of radiological, clinical, and microbiological criteria in ICU patients in MV for at least 48 h.
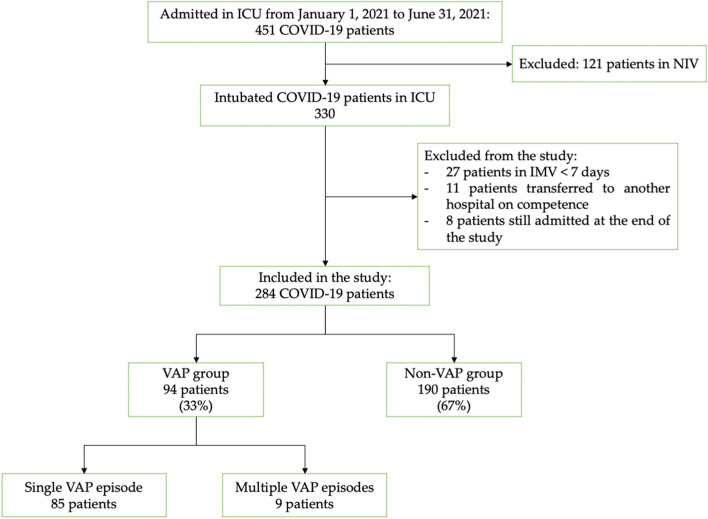
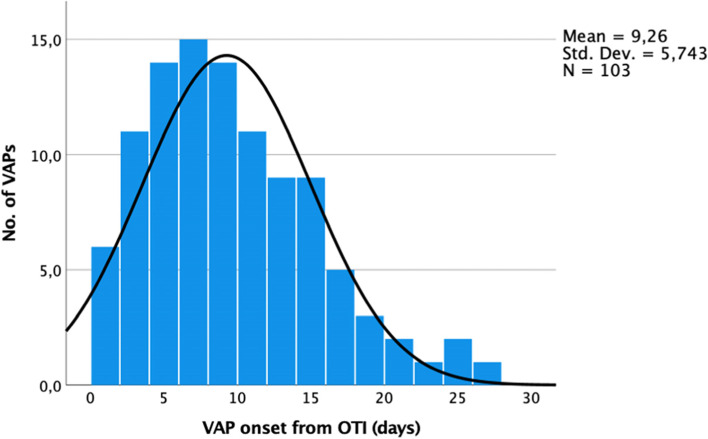
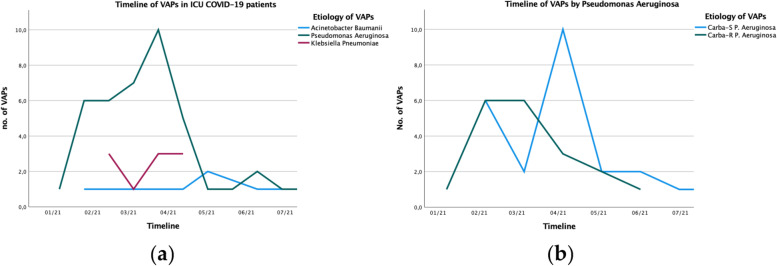
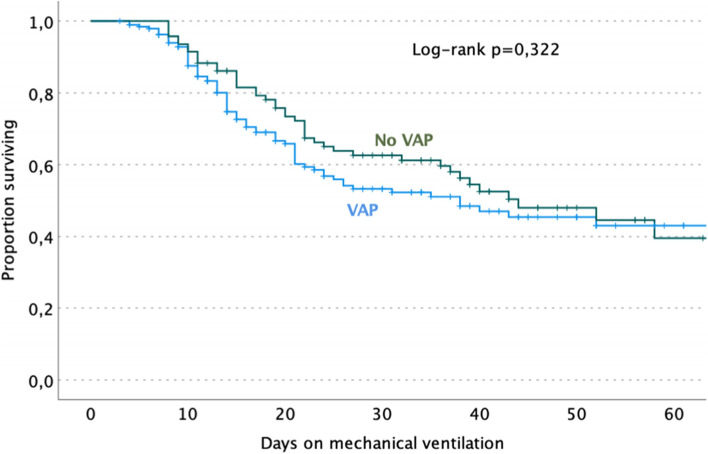
Results: Two hundred eighty-four COVID-19 patients in MV were admitted in ICU. Ninety-four patients (33%) had VAP during the ICU stay, of which 85 had a single episode of VAP and 9 multiple episodes. The median time of onset of VAP from intubation were 8 days (IQR, 5-13). The overall incidence of VAP was of 13.48 episodes per 1000 days in MV. The main etiological agent was Pseudomonas aeruginosa (39.8% of all VAPs) followed by Klebsiella spp. (16.5%); of them, 41.4% and 17.6% were carbapenem resistant, respectively. Patients during the mechanical ventilation in orotracheal intubation (OTI) had a higher incidence than those in tracheostomy, 16.46 and 9.8 episodes per 1000-MV day, respectively. An increased risk of VAP was reported in patients receiving blood transfusion (OR 2.13, 95% CI 1.26-3.59, p = 0.005) or therapy with Tocilizumab/Sarilumab (OR 2.08, 95% CI 1.12-3.84, p = 0.02). The pronation and PaO2/FiO2 ratio at ICU admission were not significantly associated with the development of VAPs. Furthermore, VAP episodes did not increase the risk of death in ICU COVID-19 patients.
Conclusions: COVID-19 patients have a higher incidence of VAP compared to the general ICU population, but it is similar to that of ICU ARDS patients in the pre-COVID-19 period. Interleukin-6 inhibitors and blood transfusions may increase the risk of VAP. The widespread use of empirical antibiotics in these patients should be avoided to reduce the selecting pressure on the growth of multidrug-resistant bacteria by implementing infection control measures and antimicrobial stewardship programs even before ICU admission.
Keywords: ARDS; Acute respiratory distress syndrome; COVID-19; Coronavirus disease 2019; Corticosteroid; Intensive care unit; Ventilator-associated pneumonia.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO Coronavirus Disease (COVID-19) Dashboard | WHO coronavirus disease (COVID-19) Dashboard Available online: https://covid19.who.int/ (Accessed on 27 May 2022).
-
- Torres A, Niederman MS, Chastre J, Ewig S, Fernandez-Vandellos P, Hanberger H, Kollef M, Li Bassi G, Luna CM, Martin-Loeches I, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur Respir J. 2017;50:1700582. doi: 10.1183/13993003.00582-2017. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous