

Predictors of intubation and mortality in COVID-19 patients: a retrospective study
- PMID: 37386623
- PMCID: PMC8626752
- DOI: 10.1186/s44158-021-00016-5
Predictors of intubation and mortality in COVID-19 patients: a retrospective study
Abstract
Background: Estimating the risk of intubation and mortality among COVID-19 patients can help clinicians triage these patients and allocate resources more efficiently. Thus, here we sought to identify the risk factors associated with intubation and intra-hospital mortality in a cohort of COVID-19 patients hospitalized due to hypoxemic acute respiratory failure (ARF).
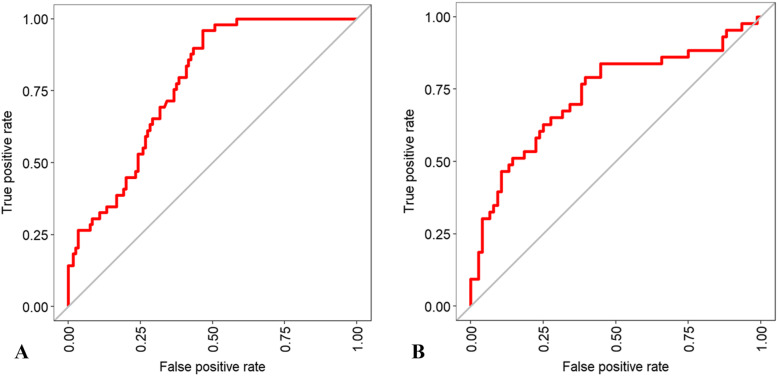
Results: We included retrospectively a total of 187 patients admitted to the subintensive and intensive care units of the University Hospital "Maggiore della Carità" of Novara between March 1st and April 30th, 2020. Based on these patients' demographic characteristics, early clinical and laboratory variables, and quantitative chest computerized tomography (CT) findings, we developed two random forest (RF) models able to predict intubation and intra-hospital mortality. Variables independently associated with intubation were C-reactive protein (p < 0.001), lactate dehydrogenase level (p = 0.018) and white blood cell count (p = 0.026), while variables independently associated with mortality were age (p < 0.001), other cardiovascular diseases (p = 0.029), C-reactive protein (p = 0.002), lactate dehydrogenase level (p = 0.018), and invasive mechanical ventilation (p = 0.001). On quantitative chest CT analysis, ground glass opacity, consolidation, and fibrosis resulted significantly associated with patient intubation and mortality. The major predictors for both models were the ratio between partial pressure of arterial oxygen and fraction of inspired oxygen, age, lactate dehydrogenase, C-reactive protein, glycemia, CT quantitative parameters, lymphocyte count, and symptom onset.
Conclusions: Altogether, our findings confirm previously reported demographic, clinical, hemato-chemical, and radiologic predictors of adverse outcome among COVID-19-associated hypoxemic ARF patients. The two newly developed RF models herein described show an overall good level of accuracy in predicting intra-hospital mortality and intubation in our study population. Thus, their future development and implementation may help not only identify patients at higher risk of deterioration more effectively but also rebalance the disproportion between resources and demand.
Keywords: COVID-19; Factor risk; Intubation; Mortality; Quantitative computerized tomography; Random forest.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures



References
-
- Renaud B, Brun-Buisson C, Santin A, Coma E, Noyez C, Fine MJ, Yealy DM, Labarere J. Outcomes of early, late, and no admission to the intensive care unit for patients hospitalized with community-acquired pneumonia. Acad Emerg Med. 2012;3(19):294–303. doi: 10.1111/j.1553-2712.2012.01301.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous