

Clot Waveform Analysis for Hemostatic Abnormalities
- PMID: 37387486
- PMCID: PMC10345169
- DOI: 10.3343/alm.2023.43.6.531
Clot Waveform Analysis for Hemostatic Abnormalities
Abstract
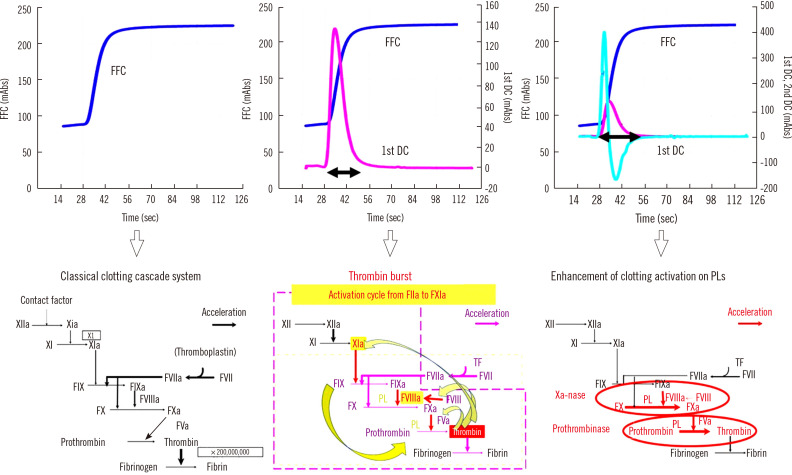
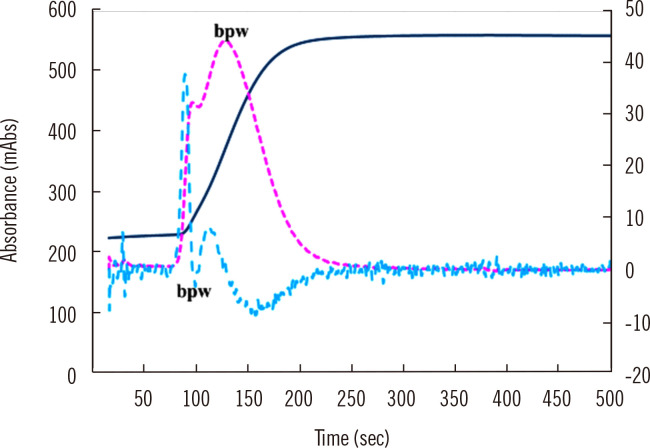
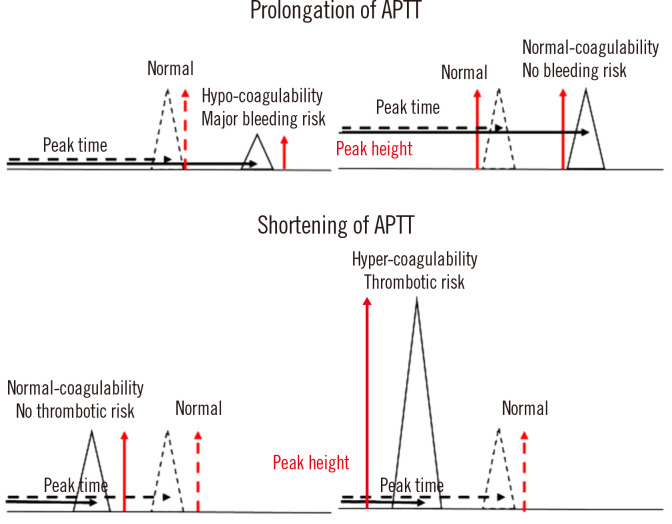
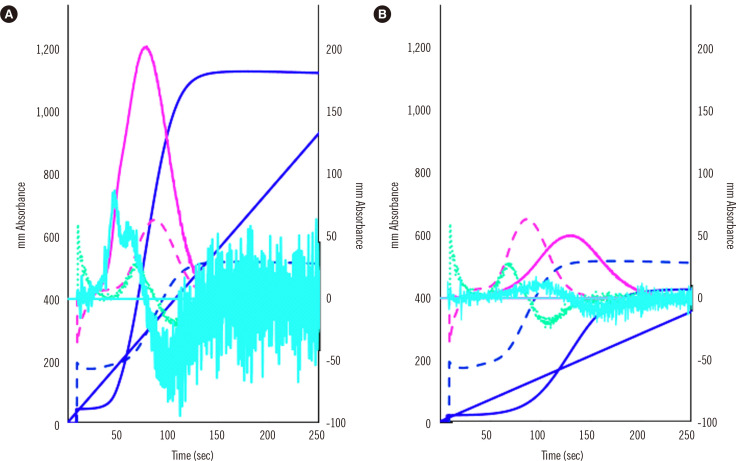
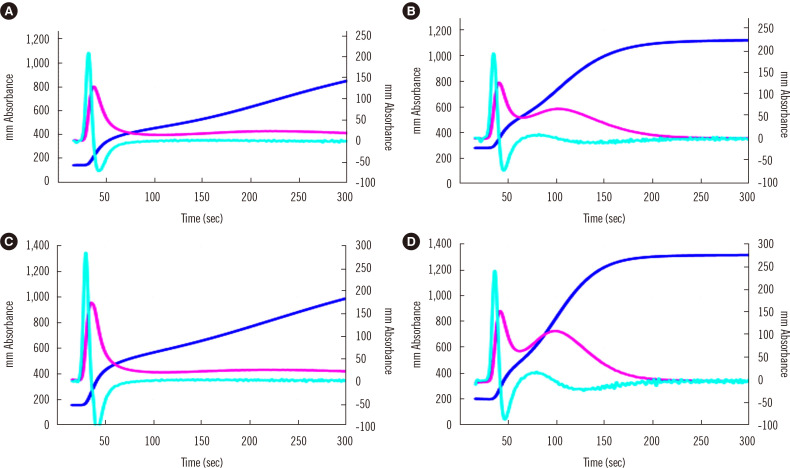
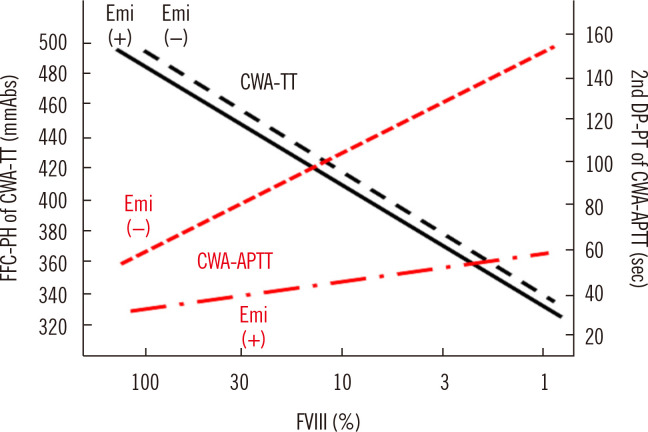
Clot waveform analysis (CWA) observes changes in transparency in a plasma sample based on clotting tests such as activated partial thromboplastin time (APTT), prothrombin time (PT), and thrombin time (TT). Evidence indicates that not only an abnormal waveform but also peak times and heights in derivative curves of CWA are useful for the evaluation of hemostatic abnormalities. Modified CWA, including the PT with APTT reagent, dilute PT (small amount of tissue factor [TF]-induced clotting factor IX [FIX] activation; sTF/FIXa), and dilute TT, has been proposed to evaluate physiological or pathological hemostasis. We review routine and modified CWA and their clinical applications. In CWA-sTF/FIXa, elevated peak heights indicate hypercoagulability in patients with cancer or thrombosis, whereas prolonged peak times indicate hypocoagulability in several conditions, including clotting factor deficiency and thrombocytopenia. CWA-dilute TT reflects the thrombin burst, whereas clot-fibrinolysis waveform analysis reflects both hemostasis and fibrinolysis. The relevance and usefulness of CWA-APTT and modified CWA should be further investigated in various diseases.
Keywords: Clot waveform analysis; Fibrinolysis; Hemostasis; Hemostatics; Indicators and reagents; Prothrombin time; Thrombin; Thrombocytopenia; Thrombophilia; Thrombosis.
Conflict of interest statement
CWA measurements were partially supported by Instrumentation Laboratory Japan (Tokyo, Japan). Further, the authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
