

Prone Vs. Supine Position Ventilation in Intubated COVID-19 Patients: A Systematic Review and Meta-Analysis
- PMID: 37388580
- PMCID: PMC10305786
- DOI: 10.7759/cureus.39636
Prone Vs. Supine Position Ventilation in Intubated COVID-19 Patients: A Systematic Review and Meta-Analysis
Abstract
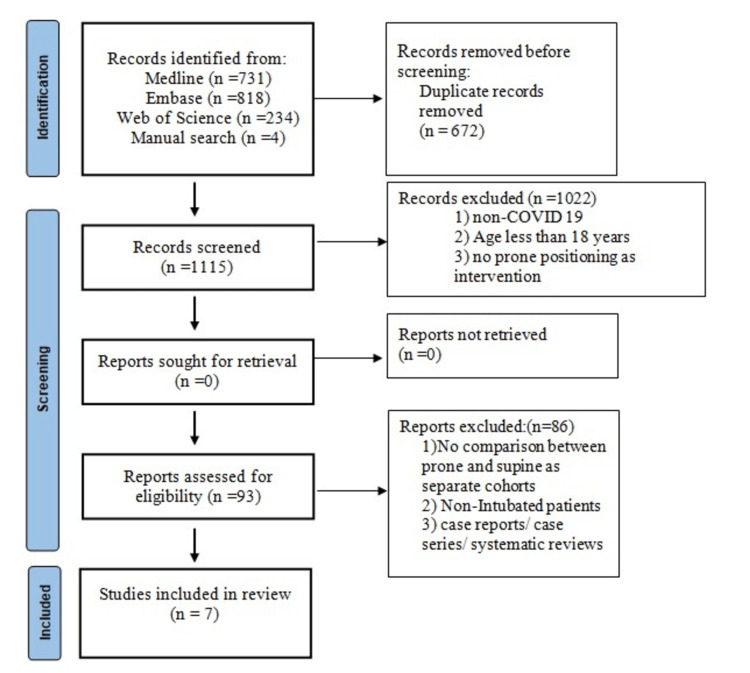
Whether prone positioning of patients undergoing mechanical ventilation for COVID-19 pneumonia has benefits over supine positioning is not clear. We conducted a systematic review with meta-analysis to determine whether prone versus supine positioning during ventilation resulted in different outcomes for patients with COVID-19 pneumonia. We searched Ovid Medline, Embase, and Web of Science for prospective and retrospective studies up through April 2023. We included studies that compared outcomes of patients with COVID-19 after ventilation in prone and supine positions. The primary outcomes were three mortality measures: hospital, overall, and intensive care unit (ICU). Secondary outcomes were mechanical ventilation days, intensive care unit (ICU) length of stay, and hospital length of stay. We conducted risk of bias analysis and used meta-analysis software to analyze results. Mean difference (MD) was used for continuous data, and odds ratio (OR) was used for dichotomous data, both with 95% CIs. Significant heterogeneity (I2) was considered if I2 was >50%. A statistically significant result was considered if the p-value was <0.05. Of 1787 articles identified, 93 were retrieved, and seven retrospective cohort studies encompassing 5216 patients with COVID-19 were analyzed. ICU mortality was significantly higher in the prone group (OR 2.22, 95% CI 1.43-3.43; p=0.0004). No statistically significant difference was observed between prone and supine groups for hospital mortality (OR, 0.95; 95% CI, 0.66-1.37; p=0.78) or overall mortality (OR, 1.08; 95% CI, 0.72-1.64; p=0.71). Studies that analyzed primary outcomes had significant heterogeneity. Hospital length of stay was significantly higher in the prone than in the supine group (MD, 6.06; 95 % CI, 3.15-8.97; p<0.0001). ICU length of stay and days of mechanical ventilation did not differ between the two groups. In conclusion, mechanical ventilation with prone positioning for all patients with COVID-19 pneumonia may not provide a mortality benefit over supine positioning.
Keywords: acute respiratory distress syndrome [ards]; covid 19; covid-19 mortality; icu mortality rate; invasive mechanical ventilation; prone positioning; severe respiratory failure; severe sepsis; supine position; systematic review and meta analysis.
Copyright © 2023, Fayed et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






References
-
- Adult respiratory distress syndrome profiles by computed tomography. Gattinoni L, Presenti A, Torresin A, et al. J Thorac Imaging. 1986;1:25–30. - PubMed
-
- Computed tomography in adult respiratory distress syndrome: what has it taught us? Pelosi P, Crotti S, Brazzi L, Gattinoni L. Eur Respir J. 1996;9:1055–1062. - PubMed
-
- An official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine clinical practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Fan E, Del Sorbo L, Goligher EC, et al. Am J Respir Crit Care Med. 2017;195:1253–1263. - PubMed
-
- Prone positioning in severe acute respiratory distress syndrome. Guérin C, Reignier J, Richard JC, et al. N Engl J Med. 2013;368:2159–2168. - PubMed
-
- Pleural pressure distribution and its relationship to lung volume and interstitial pressure. Lai-Fook SJ, Rodarte JR. J Appl Physiol (1985) 1991;70:967–978. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous