

Cost-Effectiveness of Robot-Assisted Radical Cystectomy vs Open Radical Cystectomy for Patients With Bladder Cancer
- PMID: 37389878
- PMCID: PMC10314306
- DOI: 10.1001/jamanetworkopen.2023.17255
Cost-Effectiveness of Robot-Assisted Radical Cystectomy vs Open Radical Cystectomy for Patients With Bladder Cancer
Abstract
Importance: The value to payers of robot-assisted radical cystectomy with intracorporeal urinary diversion (iRARC) when compared with open radical cystectomy (ORC) for patients with bladder cancer is unclear.
Objectives: To compare the cost-effectiveness of iRARC with that of ORC.
Design, setting, and participants: This economic evaluation used individual patient data from a randomized clinical trial at 9 surgical centers in the United Kingdom. Patients with nonmetastatic bladder cancer were recruited from March 20, 2017, to January 29, 2020. The analysis used a health service perspective and a 90-day time horizon, with supplementary analyses exploring patient benefits up to 1 year. Deterministic and probabilistic sensitivity analyses were undertaken. Data were analyzed from January 13, 2022, to March 10, 2023.
Interventions: Patients were randomized to receive either iRARC (n = 169) or ORC (n = 169).
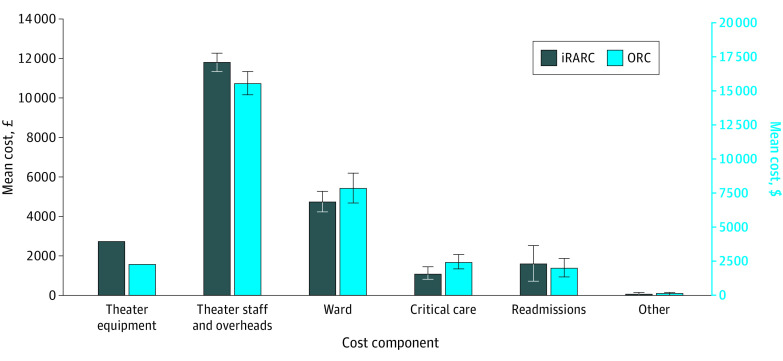
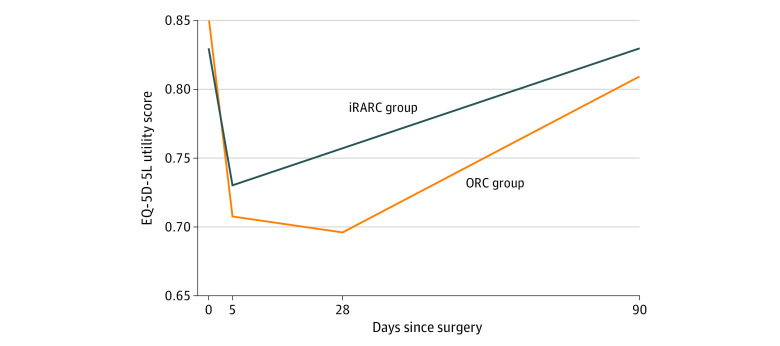
Main outcomes and measures: Costs of surgery were calculated using surgery timings and equipment costs, with other hospital data based on counts of activity. Quality-adjusted life-years were calculated from European Quality of Life 5-Dimension 5-Level instrument responses. Prespecified subgroup analyses were undertaken based on patient characteristics and type of diversion.
Results: A total of 305 patients with available outcome data were included in the analysis, with a mean (SD) age of 68.3 (8.1) years, and of whom 241 (79.0%) were men. Robot-assisted radical cystectomy was associated with statistically significant reductions in admissions to intensive therapy (6.35% [95% CI, 0.42%-12.28%]), and readmissions to hospital (14.56% [95% CI, 5.00%-24.11%]), but increases in theater time (31.35 [95% CI, 13.67-49.02] minutes). The additional cost of iRARC per patient was £1124 (95% CI, -£576 to £2824 [US $1622 (95% CI, -$831 to $4075)]) with an associated gain in quality-adjusted life-years of 0.01124 (95% CI, 0.00391-0.01857). The incremental cost-effectiveness ratio was £100 008 (US $144 312) per quality-adjusted life-year gained. Robot-assisted radical cystectomy had a much higher probability of being cost-effective for subgroups defined by age, tumor stage, and performance status.
Conclusions and relevance: In this economic evaluation of surgery for patients with bladder cancer, iRARC reduced short-term morbidity and some associated costs. While the resulting cost-effectiveness ratio was in excess of thresholds used by many publicly funded health systems, patient subgroups were identified for which iRARC had a high probability of being cost-effective.
Trial registration: ClinicalTrials.gov Identifier: NCT03049410.
Conflict of interest statement
Figures
References
-
- Vetterlein MW, Klemm J, Gild P, et al. . Improving estimates of perioperative morbidity after radical cystectomy using the European Association of Urology quality criteria for standardized reporting and introducing the Comprehensive Complication Index. Eur Urol. 2020;77(1):55-65. doi:10.1016/j.eururo.2019.08.011 - DOI - PubMed
