

Early prone positioning does not improve the outcome of patients with mild pneumonia due to SARS-CoV-2: results from an open-label randomised controlled trial - the EPCoT study
- PMID: 37389899
- PMCID: PMC10291725
- DOI: 10.1183/23120541.00181-2023
Early prone positioning does not improve the outcome of patients with mild pneumonia due to SARS-CoV-2: results from an open-label randomised controlled trial - the EPCoT study
Abstract
Background: Prone positioning is routinely used among patients with COVID-19 requiring mechanical ventilation. However, its utility among spontaneously breathing patients is still debated.
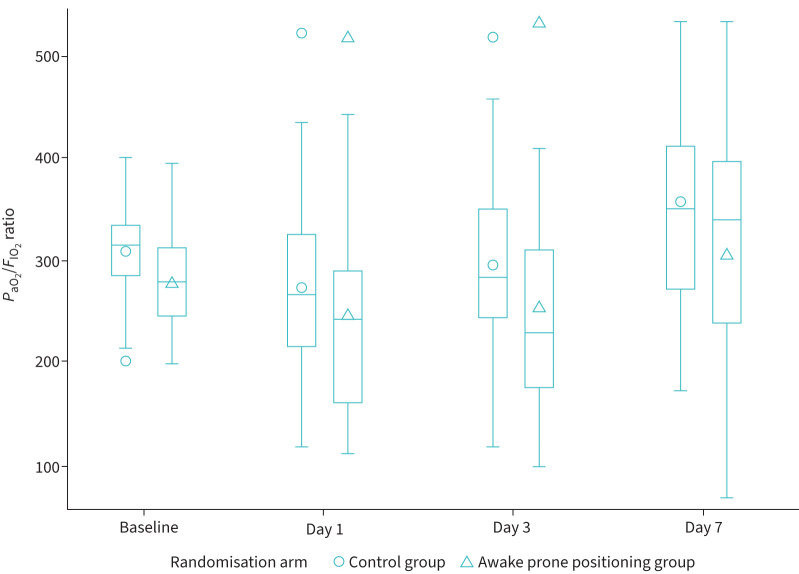
Methods: In an open-label randomised controlled trial, we enrolled patients hospitalised with mild COVID-19 pneumonia, whose arterial oxygen tension to inspiratory oxygen fraction ratio (PaO2/FIO2) was >200 mmHg and who did not require mechanical ventilation or continuous positive airway pressure at hospital admission. Patients were randomised 1:1 to prone positioning on top of standard of care (intervention group) versus standard of care only (controls). The primary composite outcome included death, mechanical ventilation, continuous positive airway pressure and PaO2/FIO2 <200 mmHg; secondary outcomes were oxygen weaning and hospital discharge.
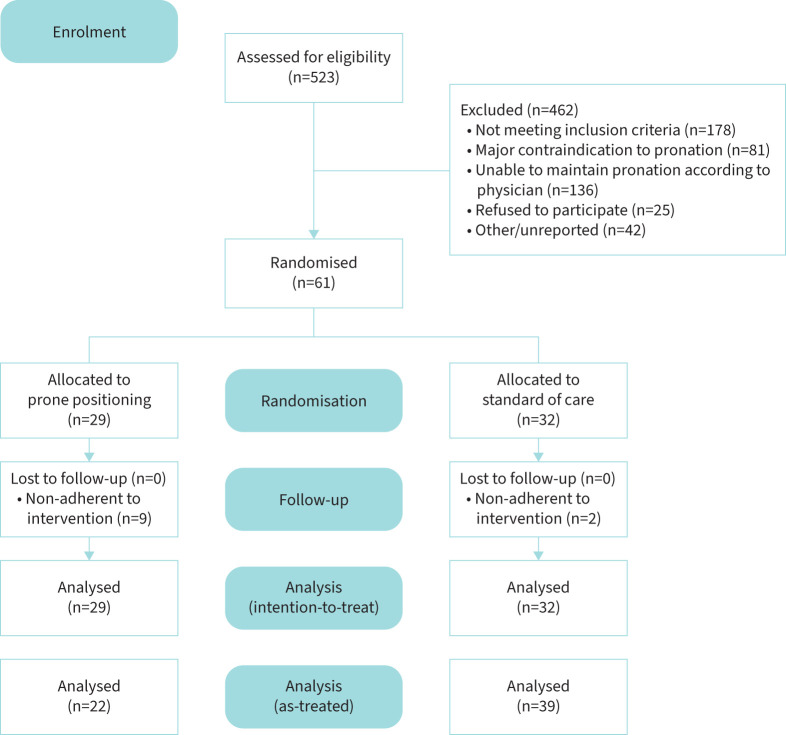
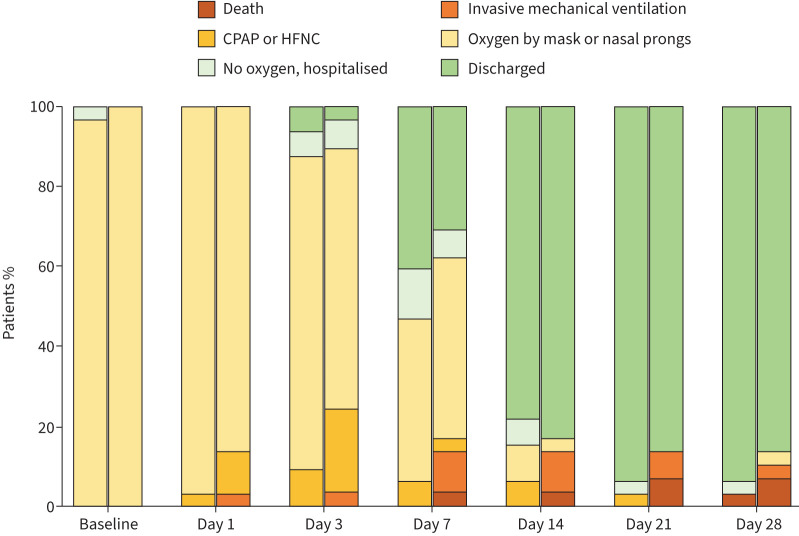
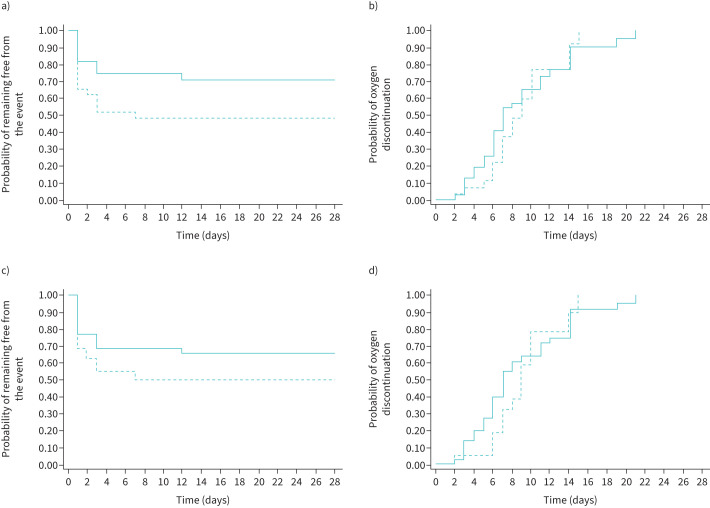
Results: A total of 61 subjects were enrolled, 29 adjudicated to prone positioning and 32 to the control group. By day 28, 24 out of 61 patients (39.3%) met the primary outcome: 16 because of a PaO2/FIO2 ratio <200 mmHg, five because of the need for continuous positive airway pressure and three because of the need for mechanical ventilation. Three patients died. Using an intention-to-treat approach, 15 out of 29 patients in the prone positioning group versus nine out of 32 controls met the primary outcome, corresponding to a significantly higher risk of progression among those randomised to prone positioning (HR 2.38, 95% CI 1.04-5.43; p=0.040). Using an as-treated approach, which included in the intervention group only patients who maintained prone positioning for ≥3 h·day-1, no significant differences were found between the two groups (HR 1.77, 95% CI 0.79-3.94; p=0.165). Also, we did not find any statistically significant difference in terms of time to oxygen weaning or hospital discharge between study arms in any of the analyses conducted.
Conclusions: We observed no clinical benefit from prone positioning among spontaneously breathing patients with COVID-19 pneumonia requiring conventional oxygen therapy.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: The authors declare that they have no conflicts of interest for the present study.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous