

Single cell transcriptomics identifies distinct profiles in pediatric acute respiratory distress syndrome
- PMID: 37391405
- PMCID: PMC10313703
- DOI: 10.1038/s41467-023-39593-0
Single cell transcriptomics identifies distinct profiles in pediatric acute respiratory distress syndrome
Abstract
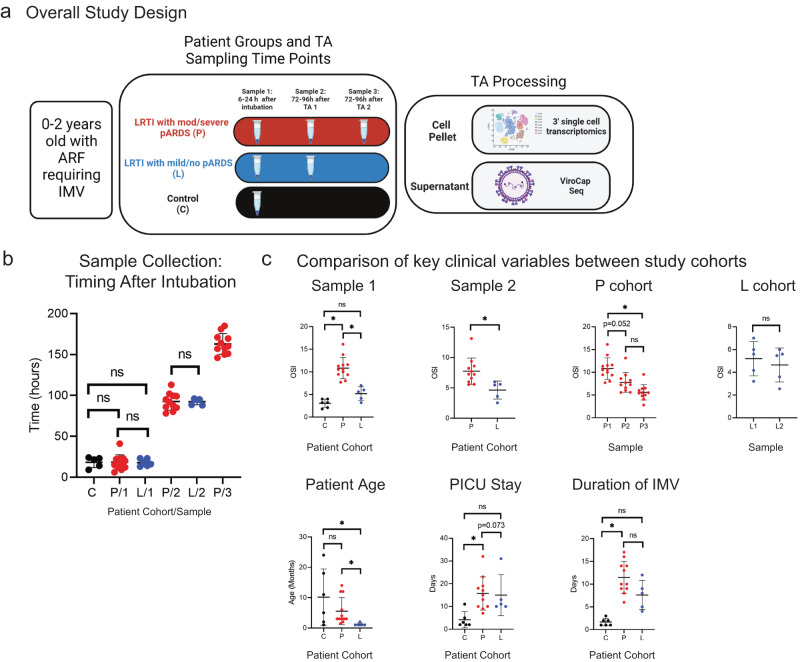
Acute respiratory distress syndrome (ARDS), termed pediatric ARDS (pARDS) in children, is a severe form of acute respiratory failure (ARF). Pathologic immune responses are implicated in pARDS pathogenesis. Here, we present a description of microbial sequencing and single cell gene expression in tracheal aspirates (TAs) obtained longitudinally from infants with ARF. We show reduced interferon stimulated gene (ISG) expression, altered mononuclear phagocyte (MNP) transcriptional programs, and progressive airway neutrophilia associated with unique transcriptional profiles in patients with moderate to severe pARDS compared to those with no or mild pARDS. We additionally show that an innate immune cell product, Folate Receptor 3 (FOLR3), is enriched in moderate or severe pARDS. Our findings demonstrate distinct inflammatory responses in pARDS that are dependent upon etiology and severity and specifically implicate reduced ISG expression, altered macrophage repair-associated transcriptional programs, and accumulation of aged neutrophils in the pathogenesis of moderate to severe pARDS caused by RSV.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
