

Long-term impact of myocardial inflammation on quantitative myocardial perfusion-a descriptive PET/MR myocarditis study
- PMID: 37391545
- PMCID: PMC10547808
- DOI: 10.1007/s00259-023-06314-0
Long-term impact of myocardial inflammation on quantitative myocardial perfusion-a descriptive PET/MR myocarditis study
Abstract
Purpose: Whether myocardial inflammation causes long-term sequelae potentially affecting myocardial blood flow (MBF) is unknown. We aimed to assess the effect of myocardial inflammation on quantitative MBF parameters, as assessed by 13N-ammonia positron emission tomography myocardial perfusion imaging (PET-MPI) late after myocarditis.
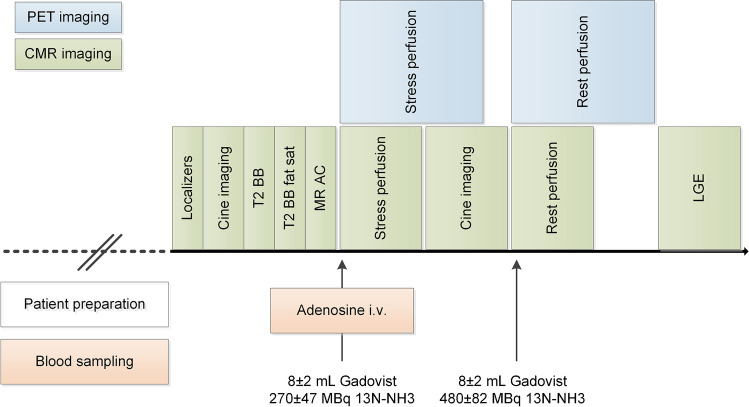
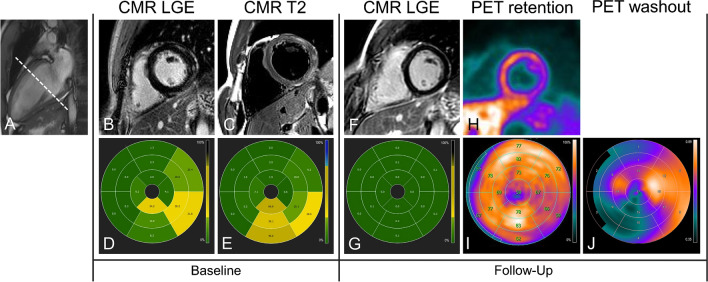
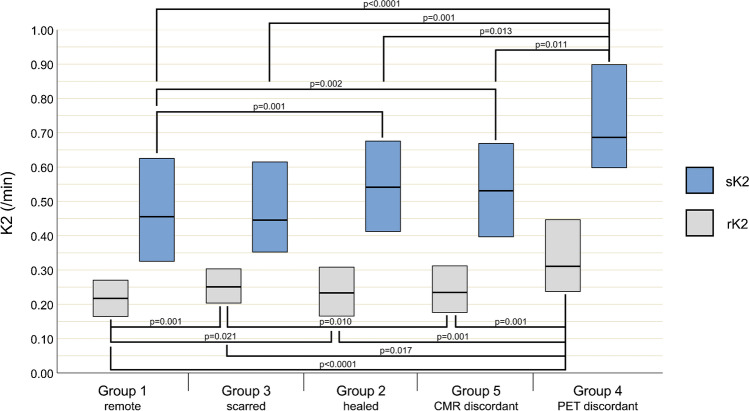
Methods: Fifty patients with a history of myocarditis underwent cardiac magnetic resonance (CMR) imaging at diagnosis and PET/MR imaging at follow-up at least 6 months later. Segmental MBF, myocardial flow reserve (MFR), and 13N-ammonia washout were obtained from PET, and segments with reduced 13N-ammonia retention, resembling scar, were recorded. Based on CMR, segments were classified as remote (n = 469), healed (inflammation at baseline but no late gadolinium enhancement [LGE] at follow-up, n = 118), and scarred (LGE at follow-up, n = 72). Additionally, apparently healed segments but with scar at PET were classified as PET discordant (n = 18).
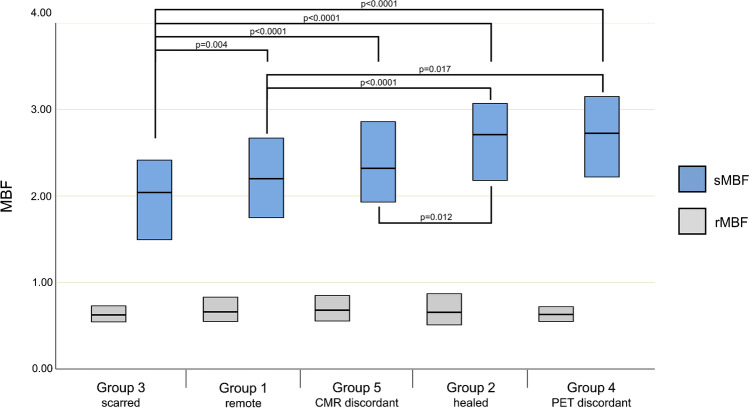
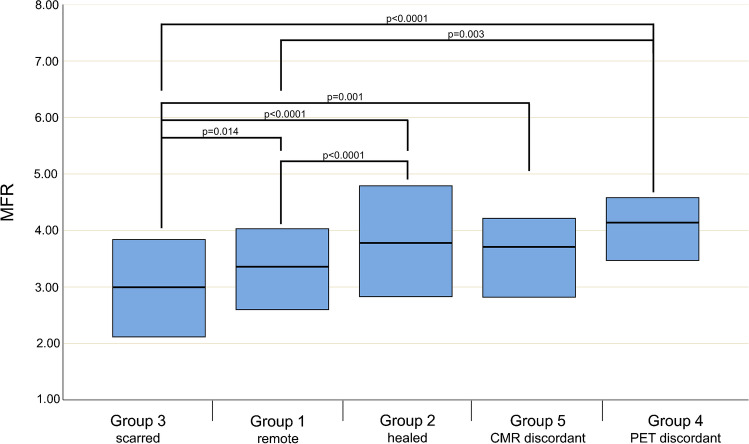
Results: Compared to remote segments, healed segments showed higher stress MBF (2.71 mL*min-1*g-1 [IQR 2.18-3.08] vs. 2.20 mL*min-1*g-1 [1.75-2.68], p < 0.0001), MFR (3.78 [2.83-4.79] vs. 3.36 [2.60-4.03], p < 0.0001), and washout (rest 0.24/min [0.18-0.31] and stress 0.53/min [0.40-0.67] vs. 0.22/min [0.16-0.27] and 0.46/min [0.32-0.63], p = 0.010 and p = 0.021, respectively). While PET discordant segments did not differ from healed segments regarding MBF and MFR, washout was higher by ~ 30% (p < 0.014). Finally, 10 (20%) patients were diagnosed by PET-MPI as presenting with a myocardial scar but without a corresponding LGE.
Conclusion: In patients with a history of myocarditis, quantitative measurements of myocardial perfusion as obtained from PET-MPI remain altered in areas initially affected by inflammation. CMR = cardiac magnetic resonance; PET = positron emission tomography; LGE = late gadolinium enhancement.
Keywords: Cardiac magnetic resonance; Inflammation; Myocardial blood flow; Myocarditis; Perfusion; Positron emission tomography.
© 2023. The Author(s).
Conflict of interest statement
The University Hospital Zurich holds a research agreement with GE Healthcare. RRB received speaker honoraria from GE Healthcare, IBA, Gilead and Pfizer. BH is inventor on patents that use RNA for diagnosis of myocarditis. Patent protection is in process for MCG for diagnosis and measurement of therapy response in inflammatory cardiomyopathy.
Figures
References
-
- Patriki D, Baltensperger N, Berg J, Cooper LT, Kissel CK, Kottwitz J, et al. A prospective pilot study to identify a myocarditis cohort who may safely resume sports activities 3 months after diagnosis. J Cardiovasc Transl Res. 2021;14(4):670–673. doi: 10.1007/s12265-020-09983-6. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
