

Worldwide variation in cardiovascular magnetic resonance practice models
- PMID: 37394485
- PMCID: PMC10316597
- DOI: 10.1186/s12968-023-00948-7
Worldwide variation in cardiovascular magnetic resonance practice models
Abstract
Introduction: The use of cardiovascular magnetic resonance (CMR) for diagnosis and management of a broad range of cardiac and vascular conditions has quickly expanded worldwide. It is essential to understand how CMR is utilized in different regions around the world and the potential practice differences between high-volume and low-volume centers.
Methods: CMR practitioners and developers from around the world were electronically surveyed by the Society for Cardiovascular Magnetic Resonance (SCMR) twice, requesting data from 2017. Both surveys were carefully merged, and the data were curated professionally by a data expert using cross-references in key questions and the specific media access control IP address. According to the United Nations classification, responses were analyzed by region and country and interpreted in the context of practice volumes and demography.
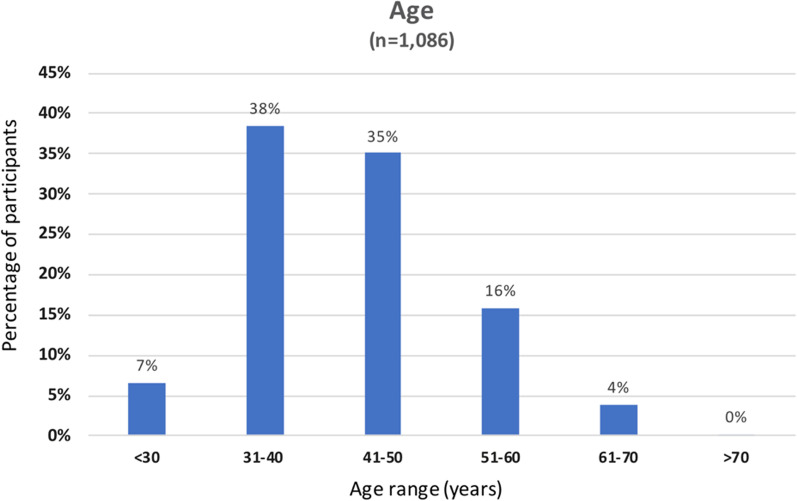
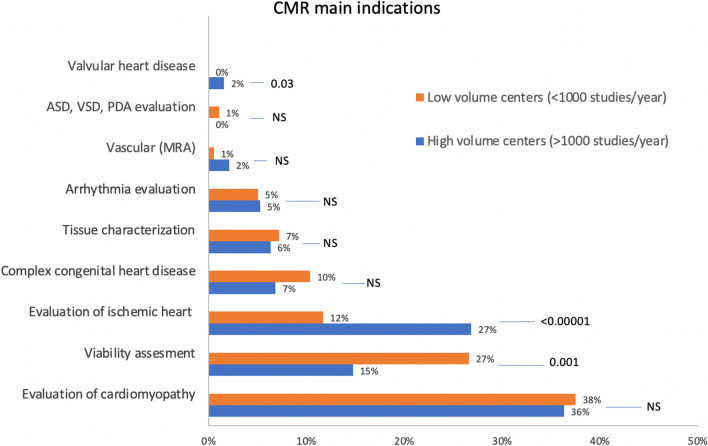
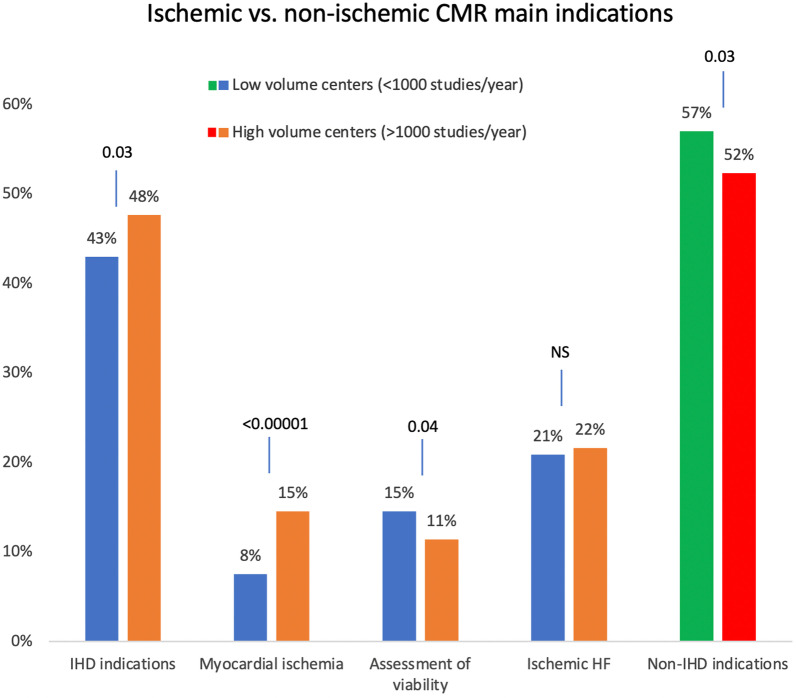
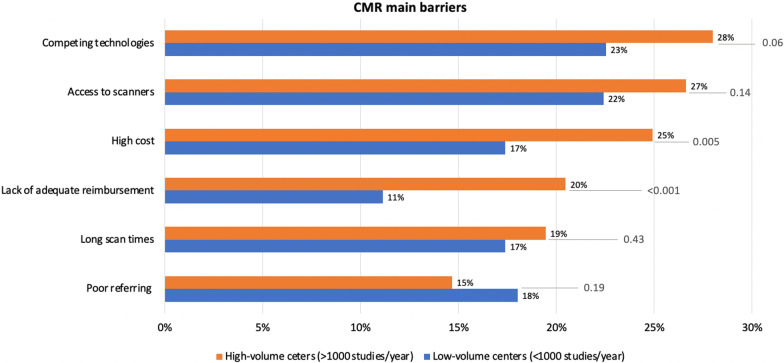
Results: From 70 countries and regions, 1092 individual responses were included. CMR was performed more often in academic (695/1014, 69%) and hospital settings (522/606, 86%), with adult cardiologists being the primary referring providers (680/818, 83%). Evaluation of cardiomyopathy was the top indication in high-volume and low-volume centers (p = 0.06). High-volume centers were significantly more likely to list evaluation of ischemic heart disease (e.g., stress CMR) as a primary indicator compared to low-volume centers (p < 0.001), while viability assessment was more commonly listed as a primary referral reason in low-volume centers (p = 0.001). Both developed and developing countries noted cost and competing technologies as top barriers to CMR growth. Access to scanners was listed as the most common barrier in developed countries (30% of responders), while lack of training (22% of responders) was the most common barrier in developing countries.
Conclusion: This is the most extensive global assessment of CMR practice to date and provides insights from different regions worldwide. We identified CMR as heavily hospital-based, with referral volumes driven primarily by adult cardiology. Indications for CMR utilization varied by center volume. Efforts to improve the adoption and utilization of CMR should include growth beyond the traditional academic, hospital-based location and an emphasis on cardiomyopathy and viability assessment in community centers.
Keywords: CMR; Cardiovascular magnetic resonance; Practice models; Survey; World.
© 2023. The Author(s).
Conflict of interest statement
LMSG has no competing interests, EESEL has no competing interests, SVR has institutional research support from Siemens, VMF receives support from the National Institute for Health Research (NIHR), Oxford Biomedical Research Centre (BRC), the British Heart Foundation (BHF), and the British Heart Foundation Centre of Research Excellence, Oxford, VR has no competing interests, EJ has no competing interests, VAF is member of the JCMR Senior Advisors Editorial Board, JSM has advisory relationships with Bayer, CWSC has no competing interests, SSMC has no competing interests, YC has no competing interests, JDLF has research agreements with Siemens AG, MT has no competing interests, TSEA has consulting and advisors relationships with Circle Cardiovascular Imaging, Inc.
Figures
References
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2022 doi: 10.1161/CIR.0000000000001063. - DOI - PubMed
-
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Eur Heart J. 2021;43(7):561–632. doi: 10.1093/eurheartj/ehab395. - DOI
-
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With. Eur Heart J. 2021;42(34):3227–3337. doi: 10.1093/eurheartj/ehab484. - DOI - PubMed
-
- 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. EP Europace, 2022;24(1):71–164. - PubMed
-
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) With the special contribution of the European Heart Rhythm Association (EHRA) Eur Heart J. 2021;42(35):3427–3520. doi: 10.1093/eurheartj/ehab364. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
