

Electrogram morphology recurrence guided catheter ablation for repeat ablation of persistent atrial fibrillation
- PMID: 37395978
- PMCID: PMC10761586
- DOI: 10.1007/s10840-023-01594-w
Electrogram morphology recurrence guided catheter ablation for repeat ablation of persistent atrial fibrillation
Abstract
Background: There are no standard mapping approaches for patients with persistent atrial fibrillation (PeAF), particularly after failed prior catheter ablation (CA). In this study, we assess the feasibility of using Electrogram Morphology Recurrence (EMR) to guide ablation.
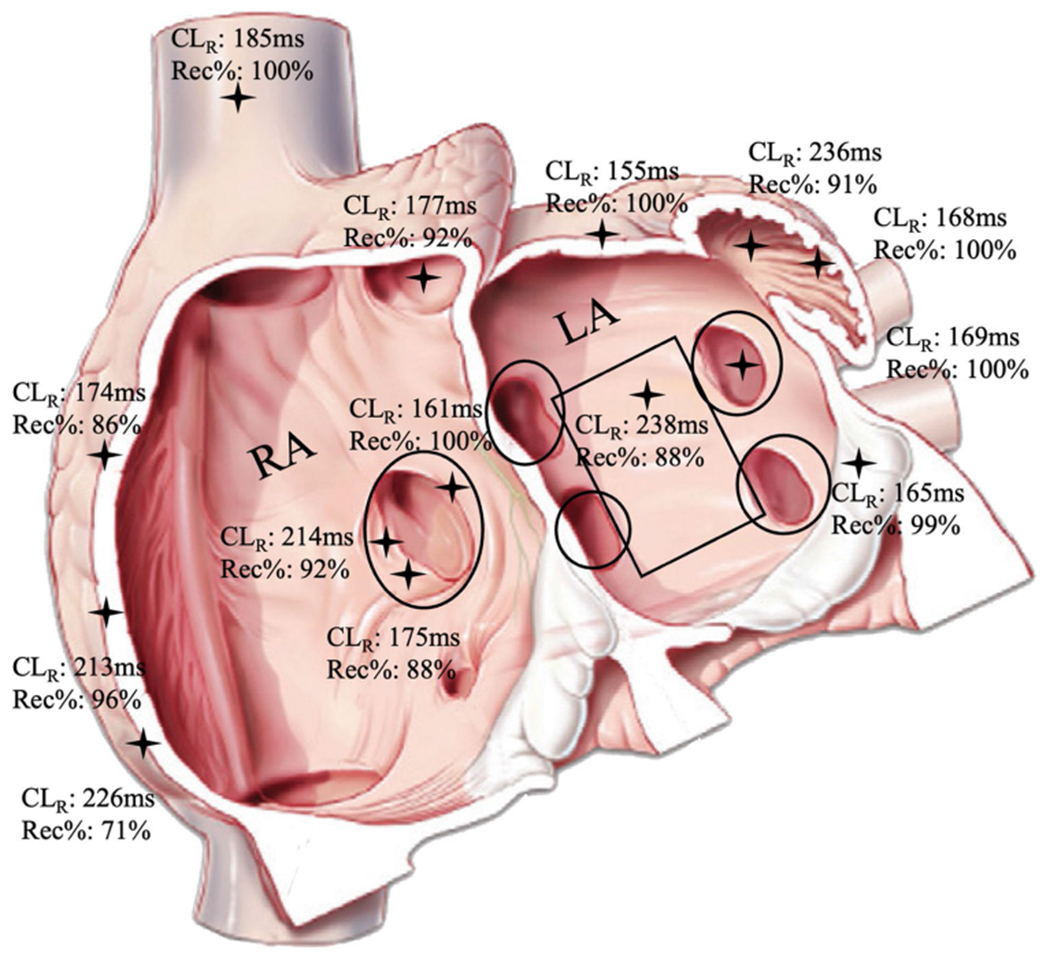
Methods: Ten patients with recurrent PeAF after prior CA underwent detailed mapping of both atria during PeAF using the PentaRay (4 mm interelectrode spacing) and 3D mapping with CARTO. At each site, 15 s recordings were made. Custom software identified each electrogram and cross-correlation was used to identify the most recurrent electrogram morphology from which the % recurrence and cycle length of the most repeatable morphology (CLR) was calculated. Sites of shortest CLR and sites within 5 ms of shortest CLR with recurrence ≥ 80% were used to inform CA strategy.
Results: A mean of 342.9 ± 131.9 LA and 328.6 ± 91.5 RA sites were recorded per patient. Nine had PV reconnection. Shortest CLR sites guided ablation in 6/10 patients while 1 patient failed to fulfill shortest CLR criteria, and another 3 did not undergo CA guided by shortest CLR due to operator preference. On 12-month follow-up, all 4 patients without shortest CLR guided CA had recurrent PeAF. Of the 6 patients with shortest CLR guided CA, 5 patients did not have recurrent PeAF (p = 0.048), although 1 had paroxysmal AF and 2 had atypical atrial flutter.
Conclusion: EMR is a feasible, novel technique to guide CA in patients with PeAF. Further evaluation is needed to provide an electrogram-based method for mapping guided targeted ablation of key areas.
Keywords: Ablation; Electrograms; Mapping; Persistent atrial fibrillation.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Figures


References
-
- Marrouche NF, Wazni O, McGann C, et al. Effect of MRI-Guided Fibrosis Ablation vs Conventional Catheter Ablation on Atrial Arrhythmia Recurrence in Patients With Persistent Atrial Fibrillation: The DECAAF II Randomized Clinical Trial. JAMA. 2022;327(23):2296–305. 10.1001/JAMA.2022.8831. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
