

Metastatic Castration-Resistant Prostate Cancer: Insights on Current Therapy and Promising Experimental Drugs
- PMID: 37396015
- PMCID: PMC10312338
- DOI: 10.2147/RRU.S385257
Metastatic Castration-Resistant Prostate Cancer: Insights on Current Therapy and Promising Experimental Drugs
Abstract
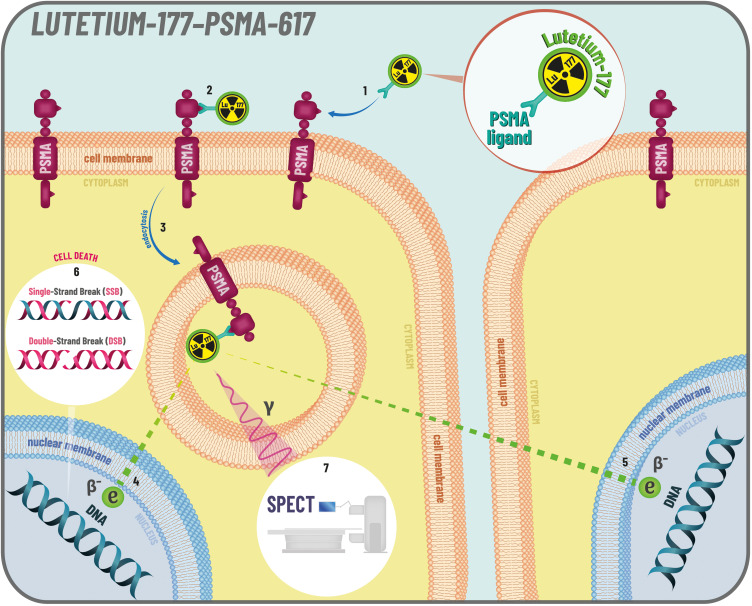
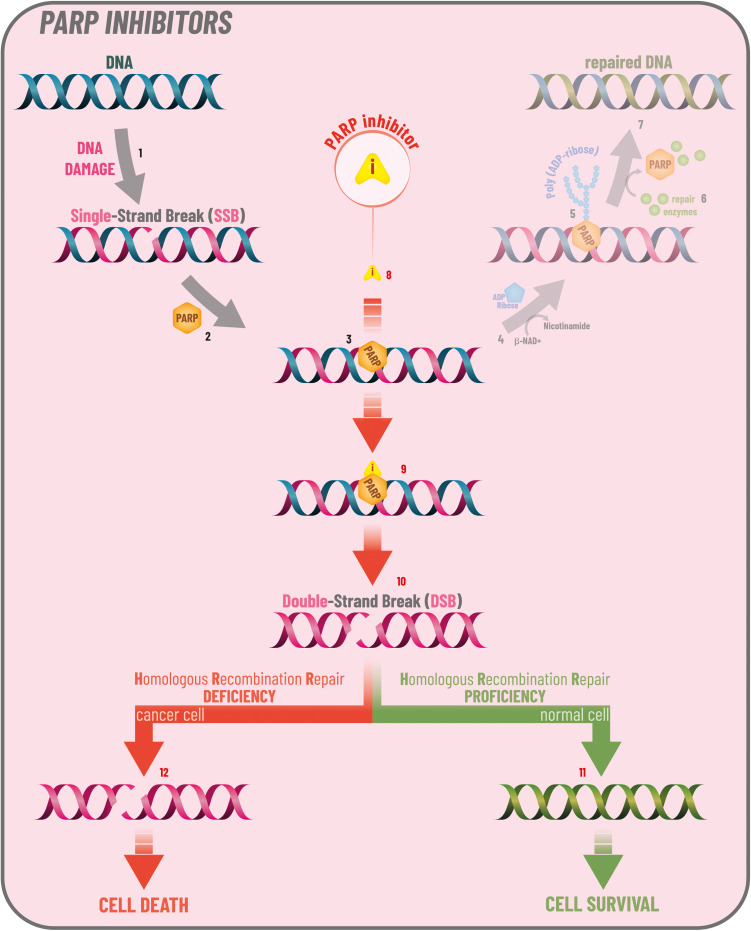
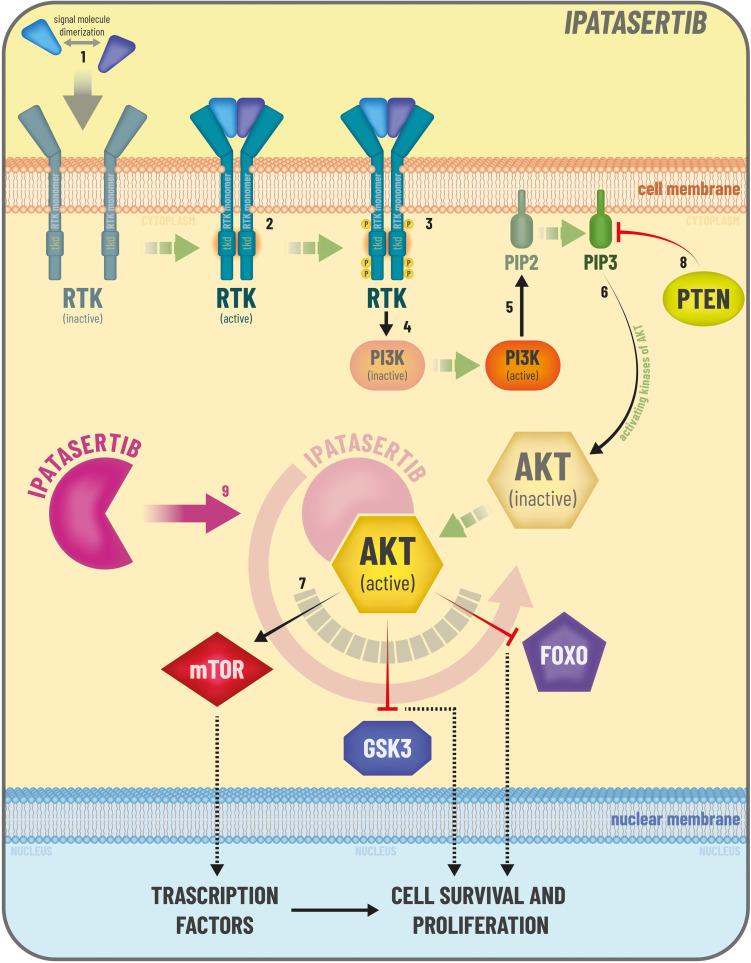
The therapeutic landscape of metastatic hormone sensitive and metastatic castration-resistant prostate cancer (mCRPC) is rapidly changing. We reviewed the current treatment options for mCRPC, with insights on new available therapeutic strategies. Chemotherapy with docetaxel or cabazitaxel (for patients progressing on docetaxel), as well as treatment with androgen receptor axis targeted therapies, and Radium-223 are well-established treatment options for patients with mCRPC. The advent of theragnostic in prostate cancer established Lutetium-177 (177Lu)-PSMA-617 as a new standard of care for PSMA-positive mCRPC previously treated with ARAT and taxane-based chemotherapy. Olaparib, a poly-ADP-ribose polymerase (PARP) inhibitor, is approved for selected patients with mCRPC progressed on ARATs and in combination with abiraterone acetate as first-line treatment for mCRPC. Immunotherapy showed limited efficacy in unselected patients with mCRPC and novel immunotherapy strategies need to be explored. The search for biomarkers is a growing field of interest in mCRPC, and predictive biomarkers are needed to support the choice of treatment and the development of tailored strategies.
Keywords: PARP inhibitors; androgen-receptors axis targeted therapies; chemotherapy; metastatic castration resistant prostate cancer; predictive biomarkers; theragnostic.
© 2023 Ferretti et al.
Conflict of interest statement
Dr Laura Marandino reports travel expenses from Janssen, personal fees for speaker compensation from Merck and Gilead, and research funding from AstraZeneca, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72:7–33. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
