

Applications of near-infrared spectroscopy in neurocritical care
- PMID: 37396062
- PMCID: PMC10311235
- DOI: 10.1117/1.NPh.10.2.023522
Applications of near-infrared spectroscopy in neurocritical care
Abstract
Significance: Acute brain injuries are commonly encountered in the intensive care unit. Alterations in cerebrovascular physiology triggered by the initial insult can lead to neurological worsening, further brain injury, and poor outcomes. Robust methods for assessing cerebrovascular physiology continuously at the bedside are limited.
Aim: In this review, we aim to assess the potential of near-infrared spectroscopy (NIRS) as a bedside tool to monitor cerebrovascular physiology in critically ill patients with acute brain injury as well as those who are at high risk for developing brain injury.
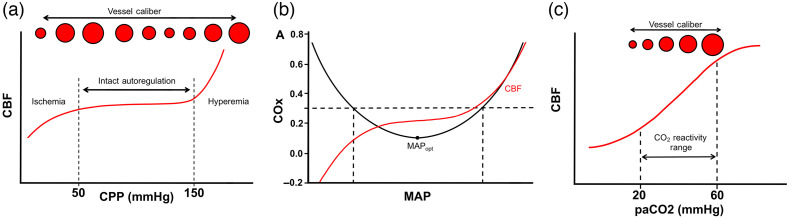
Approach: We first review basic principles of cerebral blood flow regulation and how these are altered after brain injury. We then discuss the potential role for NIRS in different acute brain injuries. We pay specific attention to the potential for NIRS to (1) identify new brain injuries and clinical worsening, (2) non-invasively measure intracranial pressure (ICP) and cerebral autoregulation, and (3) identify optimal blood pressure (BP) targets that may improve patient outcomes.
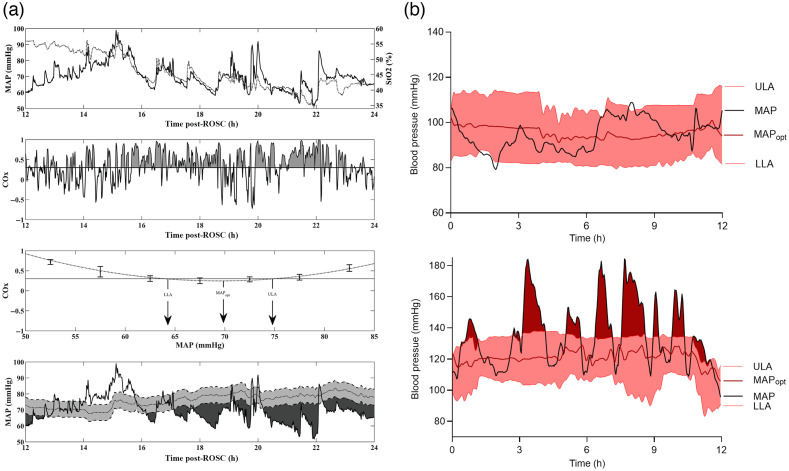
Results: A growing body of work supports the use of NIRS in the care of brain injured patients. NIRS is routinely used during cardiac surgeries to identify acute neurologic events, and there is some evidence that treatment algorithms using cerebral oximetry may result in improved outcomes. In acute brain injury, NIRS can be used to measure autoregulation to identify an "optimum" BP where autoregulation status is best preserved. Finally, NIRS has been utilized to identify oximetry thresholds that correlate with poor outcome as well as identify new focal intracranial hemorrhages.
Conclusions: NIRS is emerging as a tool that can non-invasively measure brain function in critically ill patients. Future work will be aimed at technical refinements to improve diagnostic accuracy, as well as larger scale clinical trials that can establish a definitive impact on patient outcomes.
Keywords: cerebral autoregulation; near-infrared spectroscopy; stroke; traumatic brain injury.
© 2023 The Authors.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
