

Iodine deficiency and real-life supplementation ineffectiveness in Polish pregnant women and its impact on thyroid metabolism
- PMID: 37396162
- PMCID: PMC10313195
- DOI: 10.3389/fendo.2023.1068418
Iodine deficiency and real-life supplementation ineffectiveness in Polish pregnant women and its impact on thyroid metabolism
Abstract
Introduction: Iodine is a pivotal component of thyroid hormones, and its deficiency leads to negative pregnancy outcomes. Therefore, during gestation, additional iodine supplementation is recommended.
Objectives: By evaluating a group of women from western Poland, the study updated on iodine status during pregnancy and the effectiveness of iodine supplementation in relation to the maternal and neonatal thyroid function.
Patients and methods: A total of 91 women were recruited before the delivery between 2019 and 2021. During the medical interview, the patients declared their dietary supplements intake. Thyroid parameters (TSH, ft3, ft4, a-TPO, a-Tg, and TRAb) were measured in the serum of mothers and in the cord blood of newborns after birth. Urinary iodine concentration (UIC) and urine/creatinine (UIC/crea) ratio were assessed in single urine samples using a validated high-performance liquid chromatography with ultraviolet detection (HPLC-UV). Neonatal TSH screening from dried blood spot was analyzed.
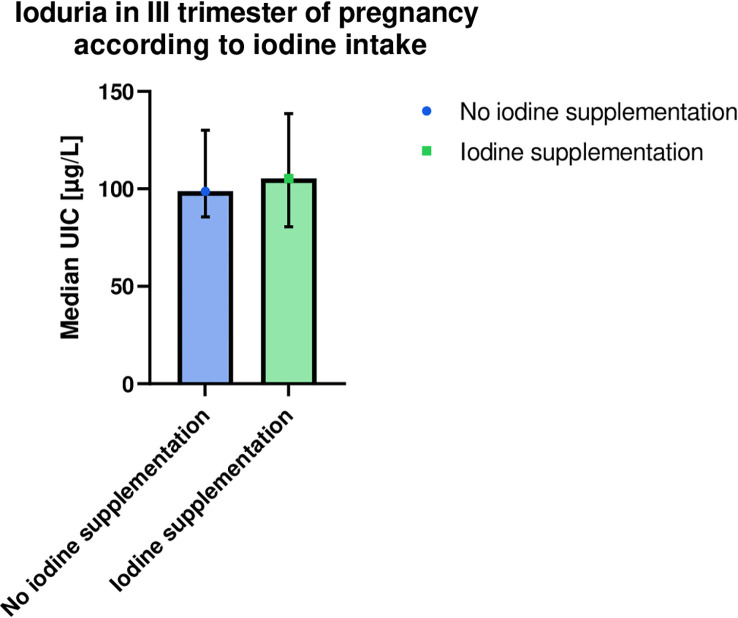
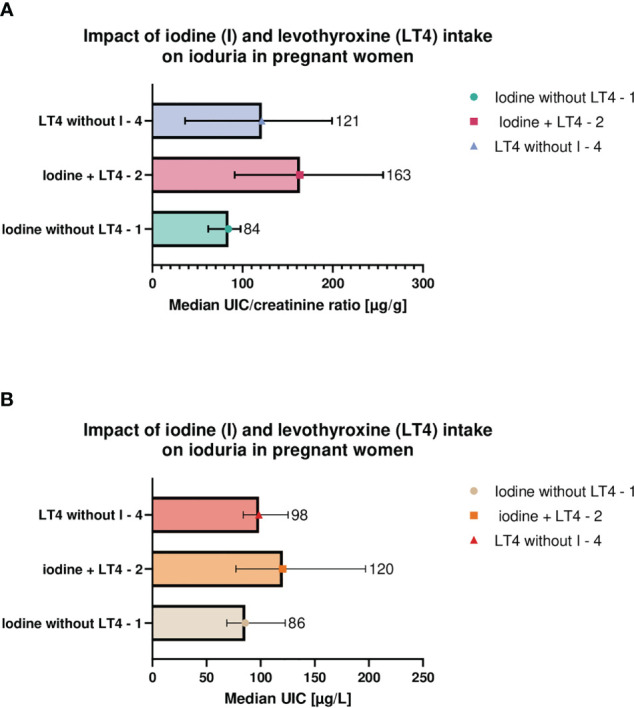
Results: Pregnant women showed a median (interquartile range) UIC of 106 (69-156) µg/liter and UIC/crea ratio of 104 (62-221) µg/g, whereas approximately 20% had UIC/crea below 50 µg/g, indicating iodine deficiency. The iodine supplementation ratio was 68%. No significant differences in UIC, UIC/crea and thyroid parameters were found between iodine supplemented and non-supplemented groups; however, the highest ioduria was detected when iodine was supplemented in addition to levothyroxine in comparison with both substances administered separately. Patients with UIC/crea within 150-249 µg/g demonstrated the lowest TSH and a-TPO levels. Screening TSH was above 5 mIU/liter in 6% of children.
Conclusions: Despite the national salt iodization and the recommendation to supplement iodine during gestation, the status of the abovementioned microelement and real-life intake revealed the ineffectiveness of the current iodine-deficiency prophylaxis model in pregnancy.
Keywords: hypothyroidism; iodine; micronutrients at pregnancy; neonatal cord blood; pregnancy supplementation guidelines; selenium; thyroiditis; urinary iodine concentration (UIC).
Copyright © 2023 Filipowicz, Szczepanek-Parulska, Mikulska-Sauermann, Karaźniewicz-Łada, Główka, Szymanowski, Ołtarzewski, Schomburg and Ruchała.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Iodine supply and thyroid function in the group of healthy pregnant women living in Warsaw].Pol Merkur Lekarski. 2013 Apr;34(202):200-4. Pol Merkur Lekarski. 2013. PMID: 23745325 Polish.
-
A randomized, double-blind study of iodine supplementation during pregnancy in Sweden: pilot evaluation of maternal iodine status and thyroid function.Eur J Nutr. 2021 Sep;60(6):3411-3422. doi: 10.1007/s00394-021-02515-1. Epub 2021 Feb 23. Eur J Nutr. 2021. PMID: 33620551 Free PMC article. Clinical Trial.
-
Iodine status of pregnant women from central Poland ten years after introduction of iodine prophylaxis programme.Endokrynol Pol. 2010 Nov-Dec;61(6):646-51. Endokrynol Pol. 2010. PMID: 21104637
-
Do maternal urinary iodine concentration or thyroid hormones within the normal range during pregnancy affect growth parameters at birth? A systematic review and meta-analysis.Nutr Rev. 2020 Sep 1;78(9):747-763. doi: 10.1093/nutrit/nuz105. Nutr Rev. 2020. PMID: 31923312
-
Relationship between mild iodine deficiency in pregnant women and thyroid function: A meta-analysis.J Trace Elem Med Biol. 2023 Jul;78:127197. doi: 10.1016/j.jtemb.2023.127197. Epub 2023 May 6. J Trace Elem Med Biol. 2023. PMID: 37209527 Review.
Cited by
-
Importance of iodide sufficiency and normal thyroid function in fertility and during gestation.Thyroid Res. 2025 May 27;18(1):22. doi: 10.1186/s13044-025-00235-w. Thyroid Res. 2025. PMID: 40420166 Free PMC article. Review.
-
Serum CD5L as potential biomarker of thyroid hormone status during pregnancy.Biofactors. 2025 Jan-Feb;51(1):e2123. doi: 10.1002/biof.2123. Epub 2024 Sep 30. Biofactors. 2025. PMID: 39345206 Free PMC article.
-
Mild-to-moderate iodine deficiency among pregnant women in Ireland: data from a large prospective pregnancy cohort.Eur J Nutr. 2025 May 9;64(4):173. doi: 10.1007/s00394-025-03692-z. Eur J Nutr. 2025. PMID: 40343500 Free PMC article.
-
Association of Mild-to-Moderate Iodine Deficiency With Thyroid Function-A Systematic Review and Meta-analysis.Adv Nutr. 2025 Jul 8;16(9):100471. doi: 10.1016/j.advnut.2025.100471. Online ahead of print. Adv Nutr. 2025. PMID: 40633808 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous