

Auxological and endocrine findings in narcolepsy type 1: seventeen-year follow-up from a pediatric endocrinology center
- PMID: 37396177
- PMCID: PMC10311432
- DOI: 10.3389/fendo.2023.1037398
Auxological and endocrine findings in narcolepsy type 1: seventeen-year follow-up from a pediatric endocrinology center
Abstract
Introduction: Narcolepsy Type 1 (NT1) is a rare hypersomnia of central origin linked to hypocretin deficiency, most frequently arising at pediatric age. NT1 could be associated with endocrine comorbidities involving the neuroendocrine axis, predominantly obesity, and Central Precocious Puberty (CPP). The primary aim of this study is the evaluation of endocrine and auxological parameters at diagnosis and during follow-up in patients with NT1, treated with Sodium Oxybate (SO) or not.
Methods: We retrospectively evaluated the auxological, biochemical, and radiological parameters of 112 patients referred to our Center between 2004-2022. The design of our study is cross-sectional at the time of diagnosis followed by a longitudinal follow-up.
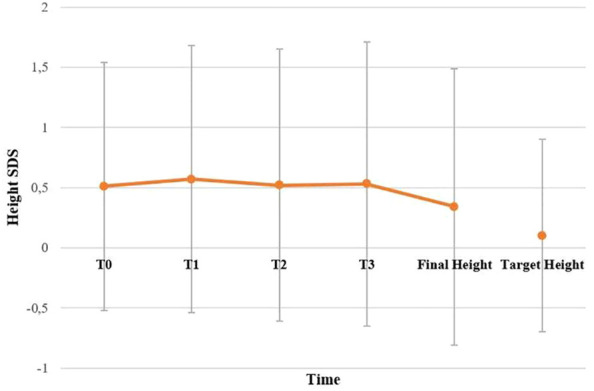
Results: Our study confirms an increased frequency of CPP and obesity in patients with NT1. At first evaluation, obesity was found in 31.3% of patients, while overweight was found in 25.0%. A diagnosis of CPP was made in 19.6% of patients. Interestingly, this group showed a significantly lower level of CSF-hypocretin (hrct-1) at diagnosis compared to others. We found an improvement in BMI SDS in the SO-treated group compared to untreated patients, and this trend persisted also at 36 months of follow-up (0.0 ± 1.3 vs 1.3 ± 0.4; p<0.03). Sixty-three patients reached their final height, with a median SDS of 0.6 ± 1.1 in boys and 0.2 ± 1.2 in girls.
Discussion: To our knowledge, these are the first results regarding the final height in a large series of pediatric patients with NT1, with a normal range of IGF1-SDS levels and stature SDS.
Keywords: central precocious puberty; final height; narcolepsy type 1; obesity; sodium oxybate.
Copyright © 2023 Casale, Assirelli, Pizza, Balsamo, Gennari, Pession, Plazzi and Cassio.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Plazzi G, Ruoff C, Lecendreux M, Dauvilliers Y, Rosen CL, Black J, et al. . Treatment of paediatric narcolepsy with sodium oxybate: a double-blind, placebo-controlled, randomised-withdrawal multicentre study and open-label investigation. Lancet Child Adolesc Health (2018) 2(7):483–94. doi: 10.1016/S2352-4642(18)30133-0 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous