

Undiagnosed chronic respiratory disorders in symptomatic patients with initially suspected and excluded coronary artery disease: insights from a prospective pilot study
- PMID: 37396893
- PMCID: PMC10310789
- DOI: 10.3389/fmed.2023.1181831
Undiagnosed chronic respiratory disorders in symptomatic patients with initially suspected and excluded coronary artery disease: insights from a prospective pilot study
Abstract
Background: Chronic respiratory diseases represent the third-leading cause of death on a global scale. Due to mutual symptoms with cardiovascular diseases and potential inappropriate attribution of symptoms, pulmonary diseases often remain undiagnosed. Therefore, we aimed to evaluate the prevalence of chronic respiratory disorders among symptomatic patients in whom suspected coronary artery disease (CAD) was ruled out.
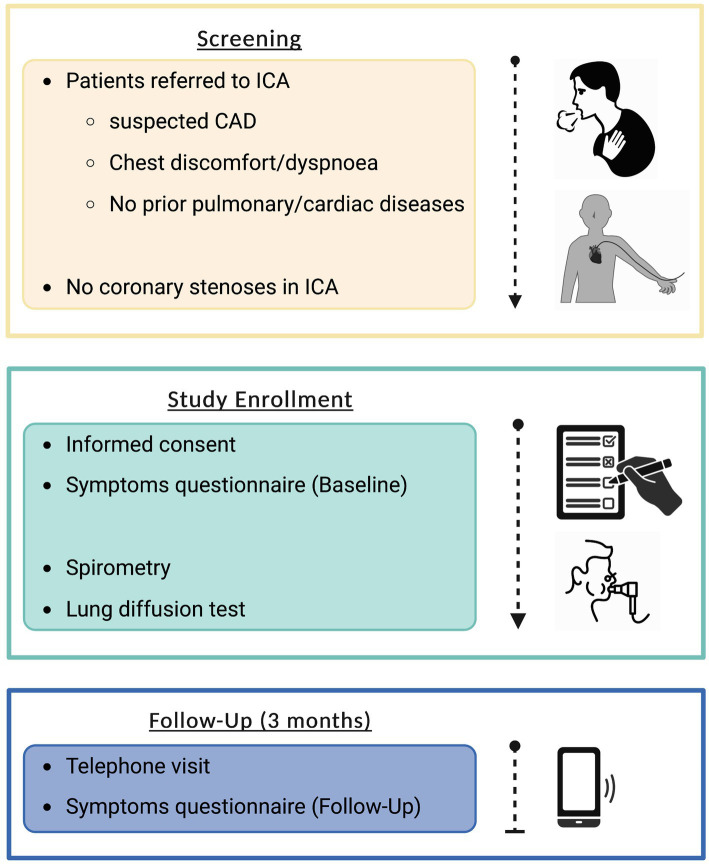
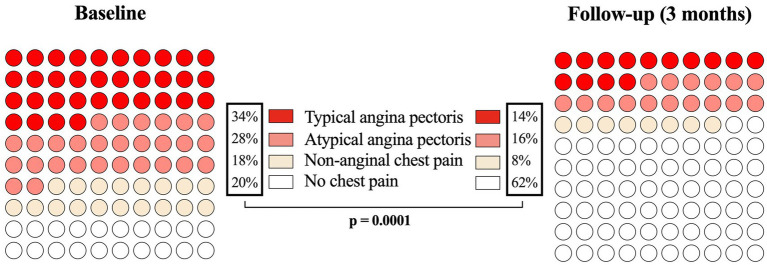
Methods: After CAD was excluded by invasive coronary angiography (ICA), 50 patients with chest pain or dyspnea were prospectively enrolled in this study. All patients underwent lung function testing, including spirometry and diffusion measurements. At baseline and the 3-month follow-up, standardized assessments of symptoms (CCS chest pain, mMRC score, CAT score) were performed.
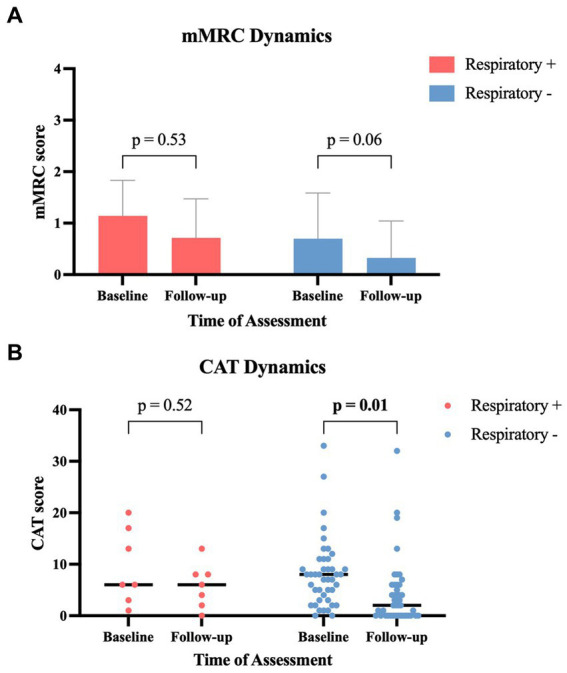
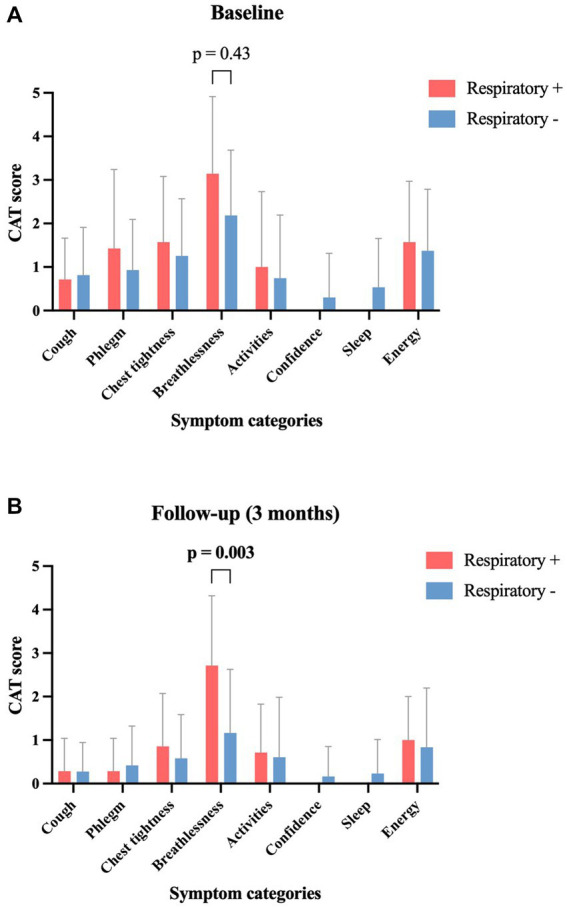
Results: Chronic respiratory disease was diagnosed in 14% of patients, with a prevalence of 6% for chronic obstructive ventilation disorders. At 3-month follow-up, patients with normal lung function tests revealed a substantial improvement in symptoms (mean mMRC 0.70 to 0.33, p = 0.06; median CAT 8 to 2, p = 0.01), while those with pulmonary findings showed non-significant alterations or unchanged symptoms (mean mMRC 1.14 to 0.71, p = 0.53; median CAT 6 to 6, p = 0.52).
Conclusion: A substantial proportion of patients with an initial suspicion of coronary artery disease was diagnosed with underlying chronic respiratory diseases and exhibited persistent symptoms.
Keywords: chest discomfort; chronic obstructive pulmonary disease; chronic respiratory disorders; coronary artery disease; dyspnea.
Copyright © 2023 Beyer, Boehm, Pizzini, Grubwieser, Feuchtner, Bauer, Weiss, Loeffler-Ragg, Friedrich and Plank.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- World Health Organization . The top 10 causes of death (2019). Available at: (https://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of...).
LinkOut - more resources
Full Text Sources
Miscellaneous