

Spinal Subdural Hematoma following Epidural Anesthesia
- PMID: 37397056
- PMCID: PMC10313436
- DOI: 10.1055/s-0043-1768576
Spinal Subdural Hematoma following Epidural Anesthesia
Abstract
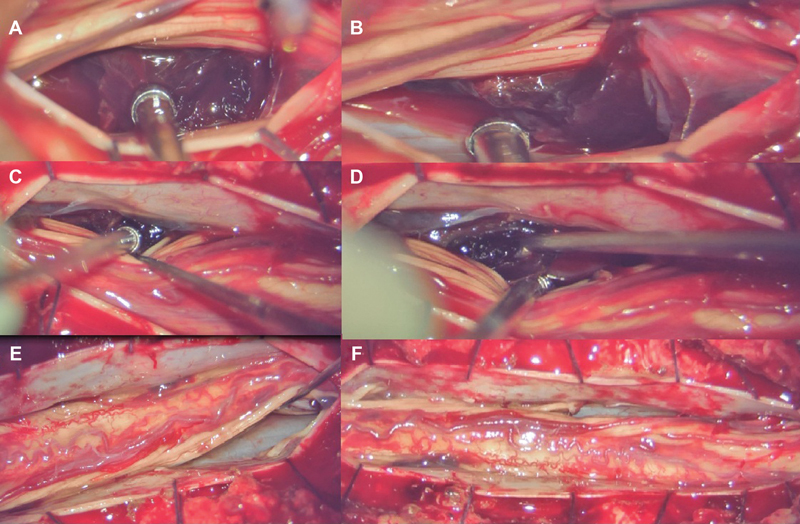
The spinal subdural space is an avascular, potential space and is a rare location for intraspinal hematomas. Compared to spinal epidural hematomas, spinal subdural hematomas are uncommonly described complications of lumbar puncture for spinal or epidural anesthesia, particularly in patients who have no pre-existing bleeding disorders or history of antiplatelet or anticoagulant intake. We describe a 19-year-old girl who had a large thoracolumbar spinal subdural hematoma following epidural anesthesia for elective cholecystectomy with no pre-existing bleeding diathesis that caused rapidly developing paraplegia that evolved over the next 2 days following surgery. Nine days after the initial surgery she underwent multilevel laminectomy and surgical evacuation with eventual satisfactory recovery. Even epidural anesthesia without thecal sac violation can result in bleeding in the spinal subdural space. The possible sources of bleed in this space may be from injury to an interdural vein or extravasation of subarachnoid bleed into the subdural space. When neurological deficits occur, prompt imaging is mandatory and early evacuation yields gratifying results.
Keywords: complications; epidural anesthesia; laminectomy; lumbar puncture; spinal subdural hematoma.
Asian Congress of Neurological Surgeons. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures


References
-
- Jackson R. Case of spinal apoplexy. Lancet. 1869;2:5–6.
-
- Kreppel D, Antoniadis G, Seeling W. Spinal hematoma: a literature survey with meta-analysis of 613 patients. Neurosurg Rev. 2003;26(01):1–49. - PubMed
Publication types
LinkOut - more resources
Full Text Sources