

Prevalence of Diastolic Dysfunction in Adult Survivors of Childhood Cancer: A Report From SJLIFE Cohort
- PMID: 37397075
- PMCID: PMC10308058
- DOI: 10.1016/j.jaccao.2022.12.010
Prevalence of Diastolic Dysfunction in Adult Survivors of Childhood Cancer: A Report From SJLIFE Cohort
Abstract
Background: The prevalence of diastolic dysfunction has not been systematically evaluated in a large population of survivors of childhood cancer using established guidelines and standards.
Objectives: This study sought to assess the prevalence and progression of diastolic dysfunction in adult survivors of childhood cancer exposed to cardiotoxic therapy.
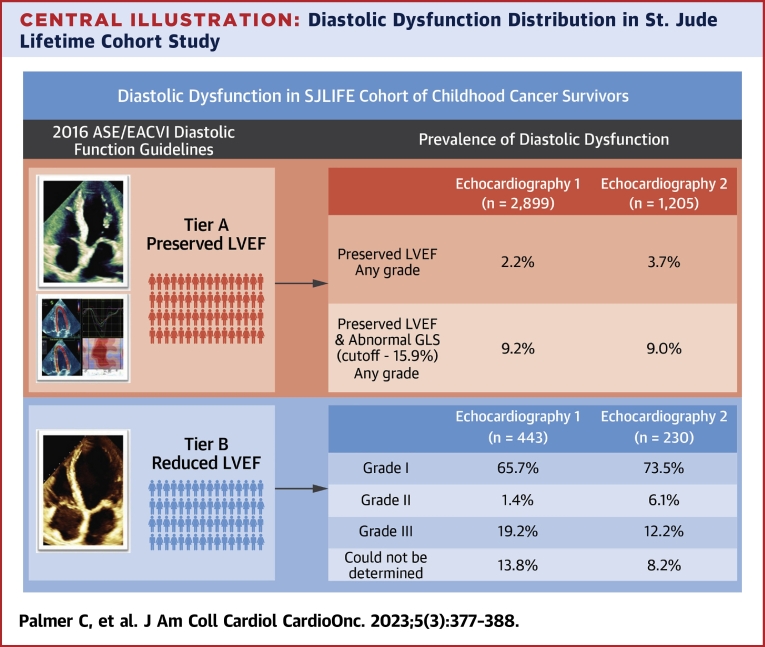
Methods: Comprehensive, longitudinal echocardiographic examinations of adult survivors of childhood cancer ≥18 years of age and ≥10 years from diagnosis in SJLIFE (St. Jude Lifetime Cohort Study) were performed. Diastolic dysfunction was defined based on 2016 American Society of Echocardiography/European Association of Cardiovascular Imaging guidelines.
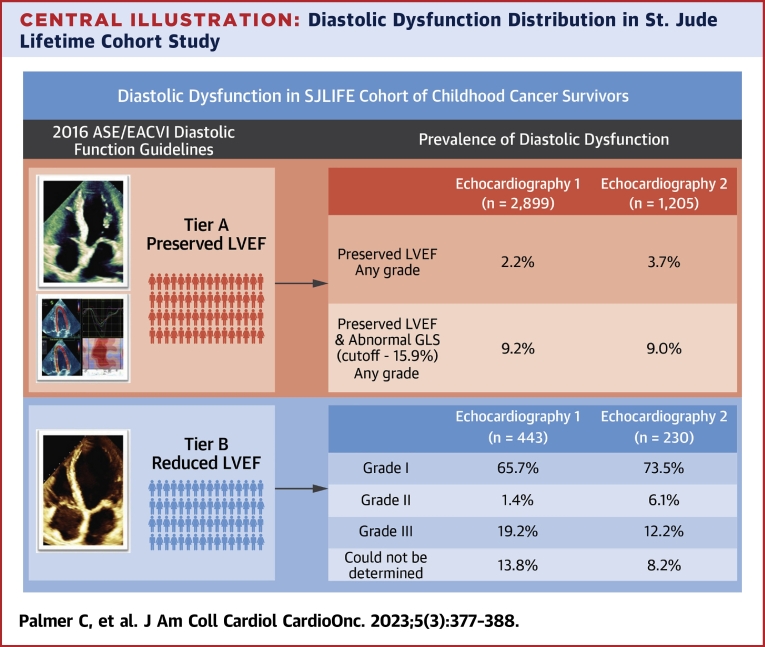
Results: Among 3,342 survivors, the median (25th-75th percentiles [quartile (Q)1-Q3]) age at diagnosis was 8.1 years (Q1-Q3: 3.6-13.7 years), 30.1 years (Q1-Q3: 24.4-37.0 years) at the baseline echocardiography evaluation (Echo 1), and 36.6 years (Q1-Q3: 30.8-43.6 years) at the last follow-up echocardiography evaluation (1,435 survivors) (Echo 2). The proportion of diastolic dysfunction was 15.2% (95% CI: 14.0%-16.4%) at Echo 1 and 15.7% (95% CI: 13.9%-17.7%) at Echo 2, largely attributable to concurrent systolic dysfunction. Less than 5% of survivors with preserved ejection fraction had diastolic dysfunction (2.2% at Echo 1, 3.7% at Echo 2). Using global longitudinal strain assessment in adult survivors with preserved ejection fraction (defined with a cutpoint worse than -15.9%), the proportion of diastolic dysfunction increased to 9.2% at baseline and 9.0% at follow-up.
Conclusions: The prevalence of isolated diastolic dysfunction is low among adults who received cardiotoxic therapies for childhood cancer. The inclusion of left ventricular global longitudinal strain significantly increased the identification of diastolic dysfunction.
Keywords: adult survivors of childhood cancer; anthracycline chemotherapy; chest-directed radiotherapy; diastolic dysfunction; echocardiography.
© 2023 The Authors.
Conflict of interest statement
Support to St. Jude Children’s Research Hospital was provided by National Cancer Institute grant U01 CA195547 (Drs Ness and Hudson [principal investigators]), the Cancer Center Support grant P30 CA21765 (Dr Roberts [principal investigator), and the American Lebanese-Syrian Associated Charities. The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Reulen R.C., Winter D.L., Frobisher C., et al. Long-term cause-specific mortality among survivors of childhood cancer. JAMA. 2010;304:172–179. - PubMed
-
- van Dalen E.C., van der Pal H.J., Kok W.E., Caron H.N., Kremer L.C. Clinical heart failure in a cohort of children treated with anthracyclines: a long-term follow-up study. Eur J Cancer. 2006;42:3191–3198. - PubMed
-
- Brouwer C.A., Postma A., Vonk J.M., et al. Systolic and diastolic dysfunction in long-term adult survivors of childhood cancer. Eur J Cancer. 2011;47:2453–2462. - PubMed
-
- Yeh E.T., Bickford C.L. Cardiovascular complications of cancer therapy: incidence, pathogenesis, diagnosis, and management. J Am Coll Cardiol. 2009;53:2231–2247. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
