

Development and validation of cancer-associated fibroblasts-related gene landscape in prognosis and immune microenvironment of bladder cancer
- PMID: 37397364
- PMCID: PMC10309557
- DOI: 10.3389/fonc.2023.1174252
Development and validation of cancer-associated fibroblasts-related gene landscape in prognosis and immune microenvironment of bladder cancer
Abstract
Backgrounds: Bladder cancer (BLCA) is one of the most prevalent cancers of the genitourinary system, the clinical outcomes of patients with BLCA are bad, and the morbidity rate is high. One of the key components of the tumor microenvironment (TME) is cancer-associated fibroblasts (CAFs) which are critically involved in BLCA tumorigenesis. Previous studies have shown the involvement of CAFs in tumor growth, cancer progression, immune evasion, angiogenesis, and chemoresistance in several cancers such as breast, colon, pancreatic, ovarian, and prostate cancers. However, only a few studies have shown the role of CAFs in the occurrence and development of BLCA.
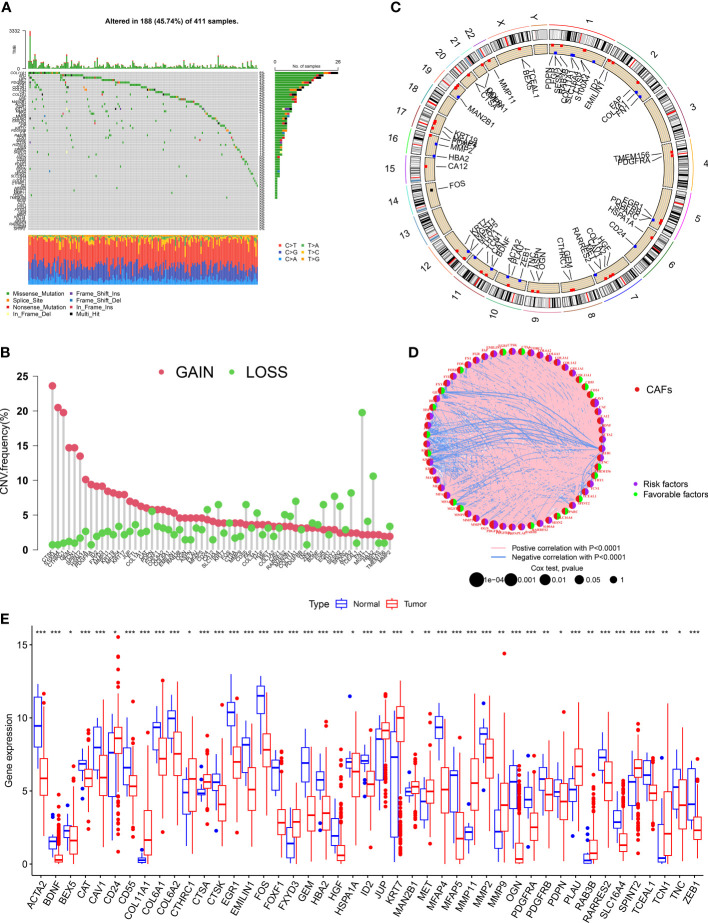
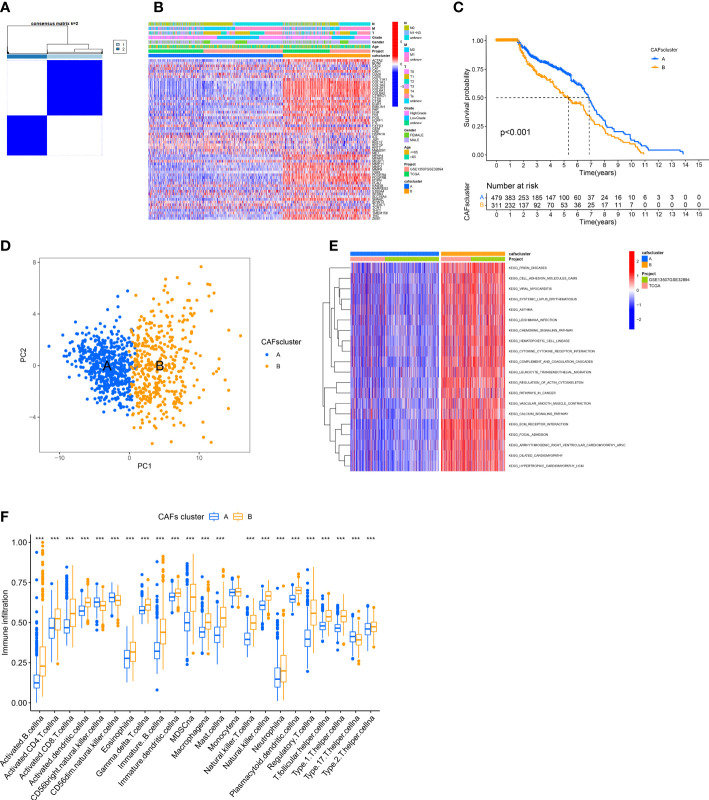
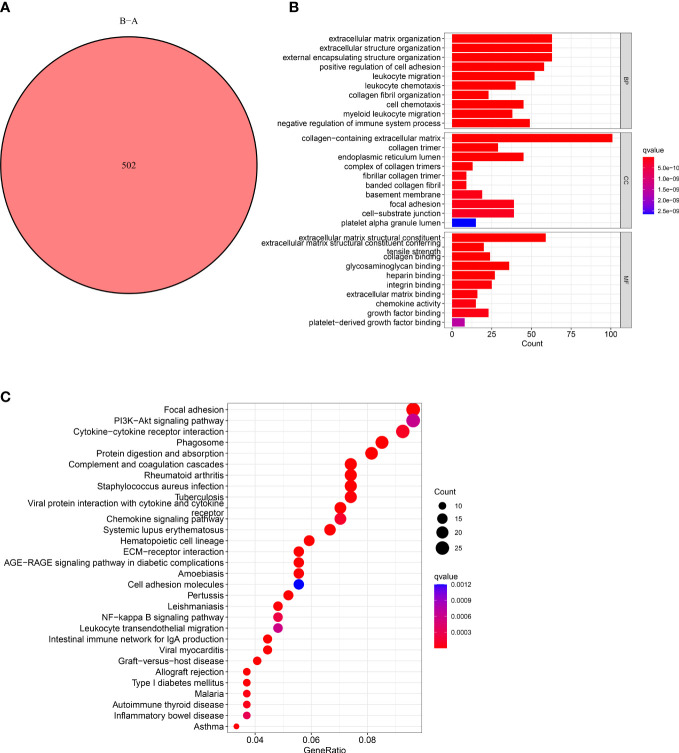
Methods: We have retrieved and merged the data on RNA-sequencing of patients with BLCA from databases including "the Cancer Genome Atlas" and "Gene Expression Omnibus." Next, we compared the differences in CAFs-related genes (CRGs) expression between normal and BLCA tissues. Based on CRGs expression, we randomly divided patients into two groups. Next, we determined the correlation between CAFs subtypes and differentially expressed CRGs (DECRGs) between the two subtypes. Furthermore, the "Gene Ontology" and "Kyoto Encyclopedia of Genes and Genomes pathway" enrichment analyses were conducted to determine the functional characteristics between the DECRGs and clinicopathology.
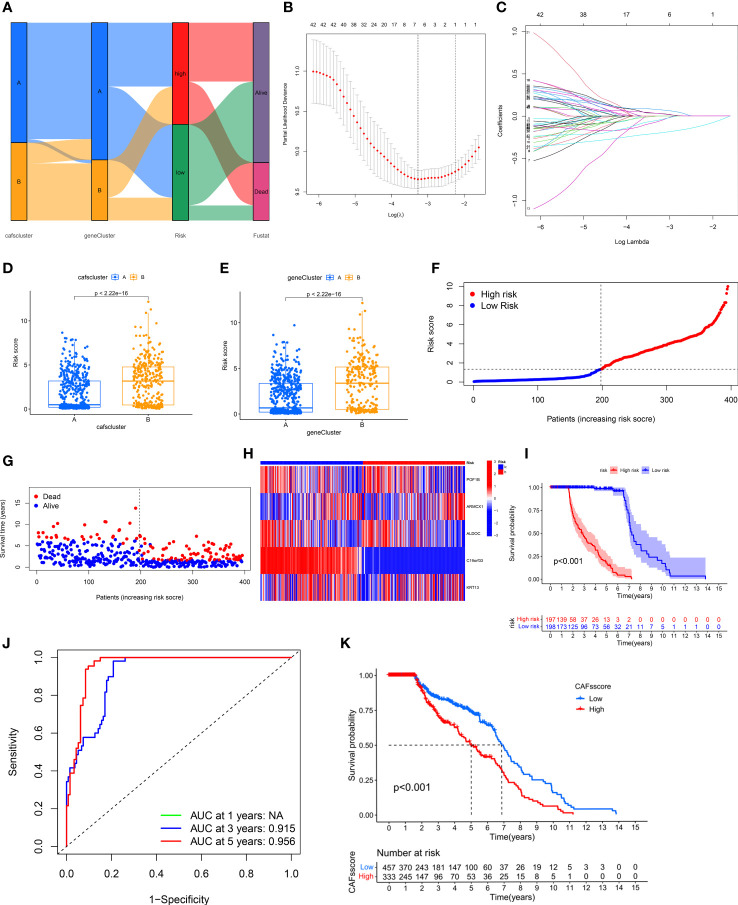
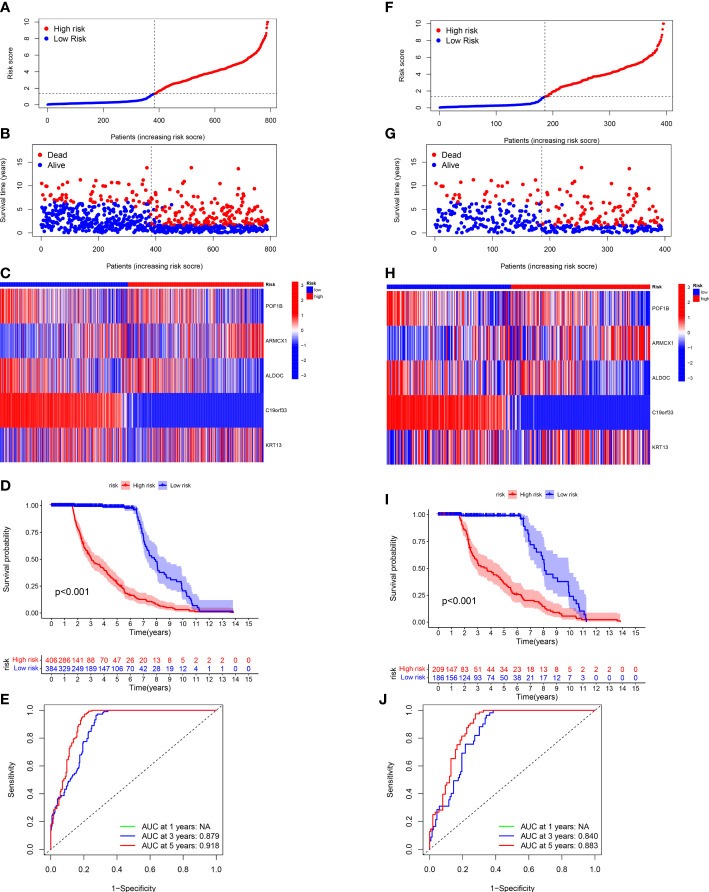
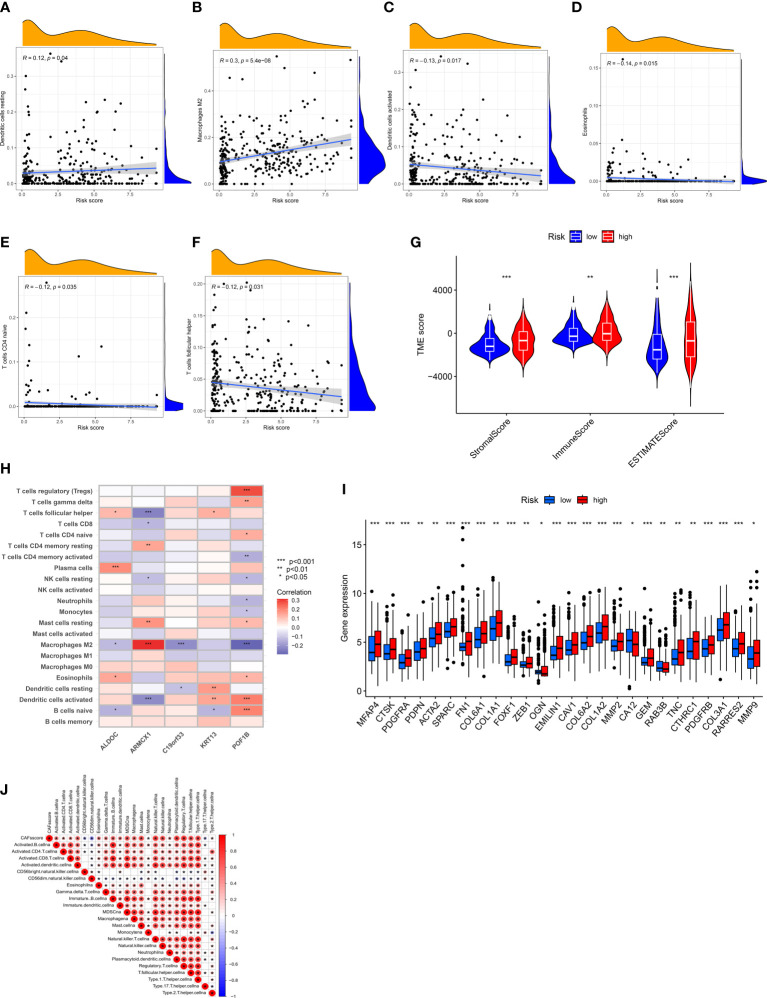
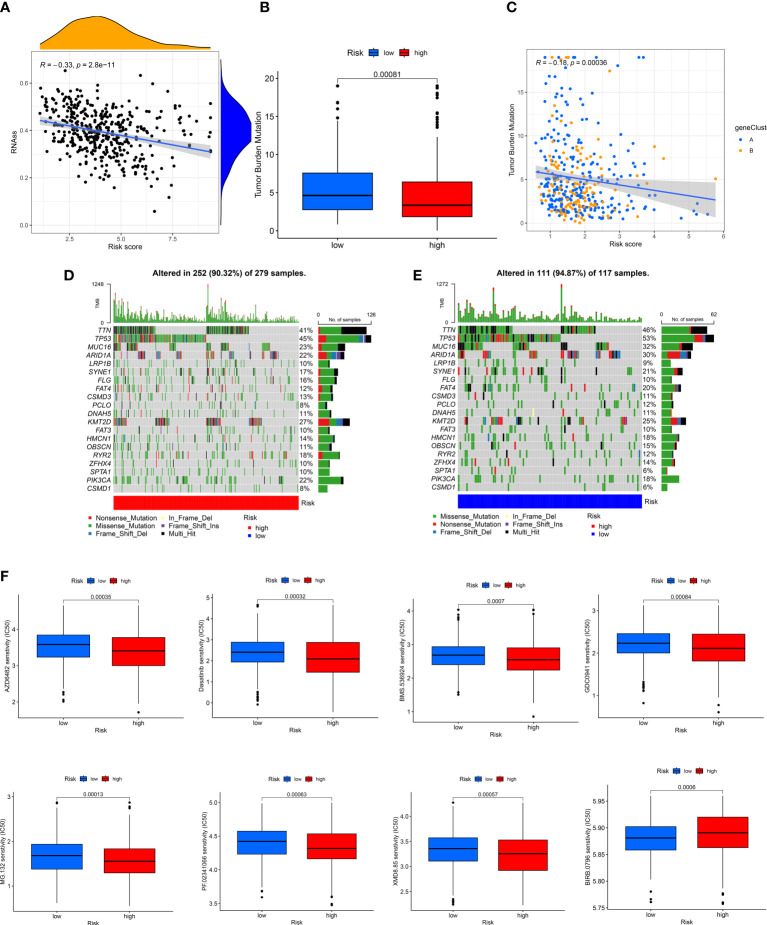
Results: We identified five genes (POF1B, ARMCX1, ALDOC, C19orf33, and KRT13) using multivariate COX regression and "Least Absolute Shrinkage and Selection Operator (LASSO) COX regression analysis" for developing a prognostic model and calculating the CRGs-risk score. The TME, mutation, CSC index, and drug sensitivity were also analyzed.
Conclusion: We constructed a novel five- CRGs prognostic model, which sheds light on the roles of CAFs in BLCA.
Keywords: bladder cancer; cancer-associated fibroblasts (CAF); immune microenvironment; prognosis; tumor microenvironment.
Copyright © 2023 Zhang, Zhu, Zhang, Li, Min, Li and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous