

PLSCR1 promotes apoptosis and clearance of retinal ganglion cells in glaucoma pathogenesis
- PMID: 37397520
- PMCID: PMC10311034
- DOI: 10.1016/j.gendis.2022.05.036
PLSCR1 promotes apoptosis and clearance of retinal ganglion cells in glaucoma pathogenesis
Abstract
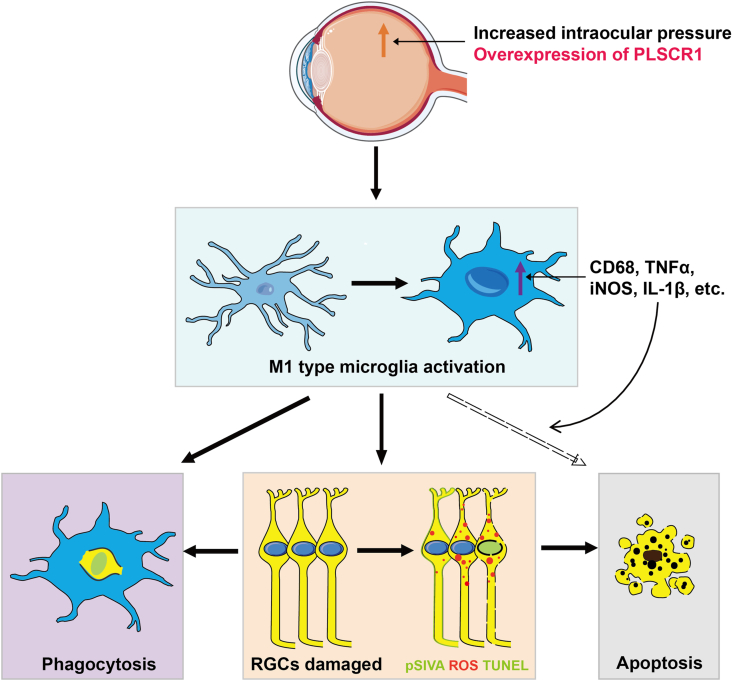
Glaucoma is the leading cause of irreversible blindness worldwide. In the pathogenesis of glaucoma, activated microglia can lead to retinal ganglion cells (RGCs) apoptosis and death, however, the molecular mechanisms remain largely unknown. We demonstrate that phospholipid scramblase 1 (PLSCR1) is a key regulator promoting RGCs apoptosis and their clearance by microglia. As evidenced in retinal progenitor cells and RGCs of the acute ocular hypertension (AOH) mouse model, overexpressed PLSCR1 induced its translocation from the nucleus to the cytoplasm and cytomembrane, as well as elevated phosphatidylserine exposure and reactive oxygen species generation with subsequent RGCs apoptosis and death. These damages were effectively attenuated by PLSCR1 inhibition. In the AOH model, PLSCR1 led to an increase in M1 type microglia activation and retinal neuroinflammation. Upregulation of PLSCR1 resulted in strongly elevated phagocytosis of apoptotic RGCs by activated microglia. Taken together, our study provides important insights linking activated microglia to RGCs death in the glaucoma pathogenesis and other RGC-related neurodegenerative diseases.
Keywords: Apoptosis; Glaucoma; PLSCR1; Phagocytosis; Retinal ganglion cells.
© 2022 The Authors. Publishing services by Elsevier B.V. on behalf of KeAi Communications Co., Ltd.
Figures







References
-
- Quigley H.A. Glaucoma. Lancet. 2011;377(9774):1367–1377. - PubMed
-
- Silverman S.M., Wong W.T. Microglia in the retina: roles in development, maturity, and disease. Annu Rev Vis Sci. 2018;4:45–77. - PubMed
-
- Baudouin C., Kolko M., Melik-Parsadaniantz S., Messmer E.M. Inflammation in Glaucoma: from the back to the front of the eye, and beyond. Prog Retin Eye Res. 2021;83 - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
