

Trends in the use of benzodiazepine receptor agonists among working-age adults in Belgium from 2004 to 2018
- PMID: 37397739
- PMCID: PMC10311493
- DOI: 10.3389/fpubh.2023.1191151
Trends in the use of benzodiazepine receptor agonists among working-age adults in Belgium from 2004 to 2018
Abstract
Introduction: The use of psychotropics, such as benzodiazepine receptor agonists (BzRAs), among working-age adults in Belgium has shown educational differences. However, it is unclear how work status plays a role in this relationship. Therefore, this research aims to investigate whether work status explains observed educational differences in BzRA use. In addition, considering medicalisation processes, where non-medical factors, such as work status, are increasingly associated with medical mental health care-seeking behavior, this research also aims to investigate whether work status explains observed educational differences in BzRA use, regardless of mental health status.
Methods: Data are obtained from the Belgian Health Interview Survey (BHIS). Four successive waves are covered: 2004, 2008, 2013, and 2018. The weighted data represent a sample of 18,547 Belgian respondents aged 18 to 65 years old. Poisson regression models are used to analyze the research aims. Time evolutions are plotted using marginal means postestimation.
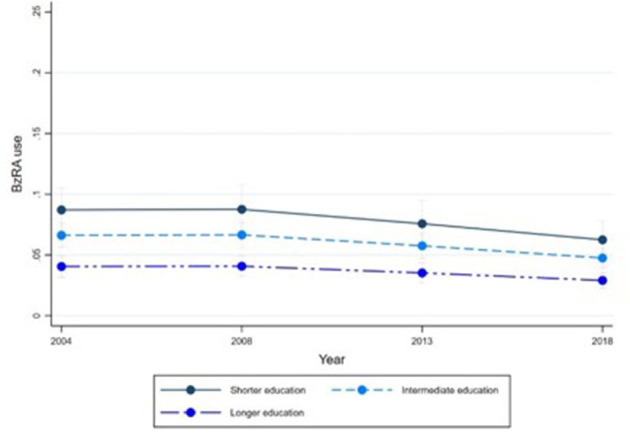
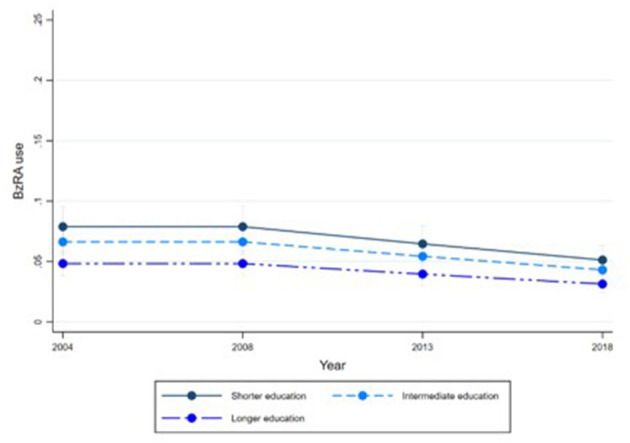
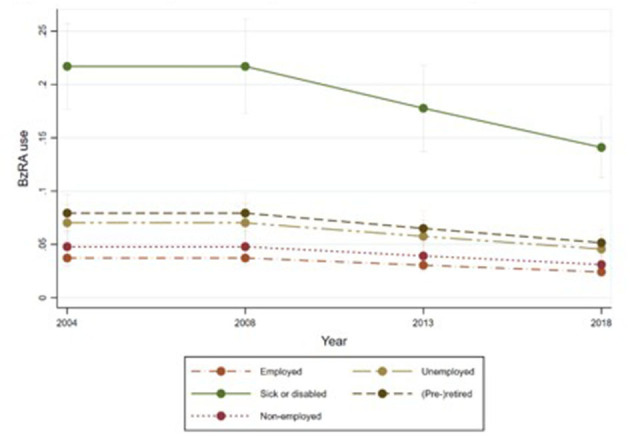
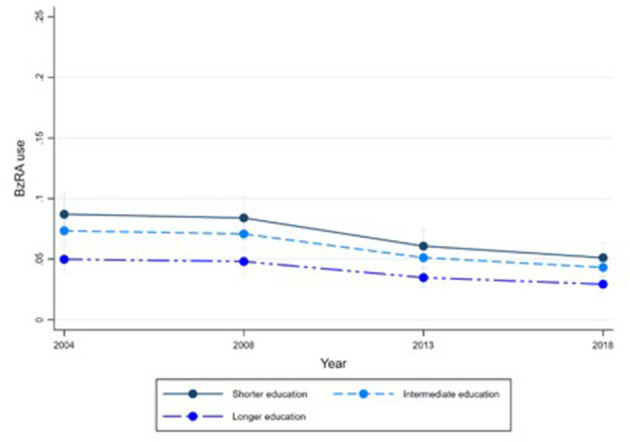
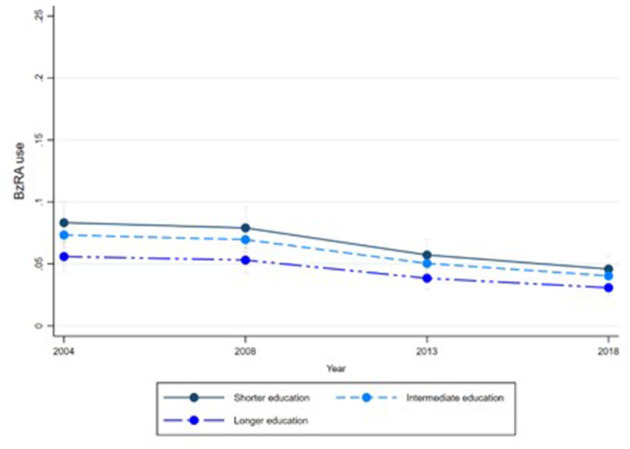
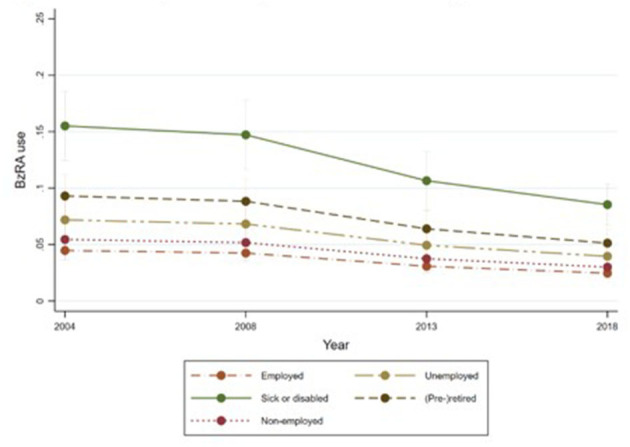
Results: The average use of BzRAs shows a slight decline over the waves studied (2004 = 5.99, 2008 = 5.88, 2013 = 5.33, 2018 = 4.31). Educational and work status differences in BzRA use are observed, regardless of mental health status. Individuals with longer education report lower use compared to individuals with shorter education, and individuals who are unemployed, (pre-)retired, or sick or disabled report higher use compared to employed individuals. Furthermore, work status acts as a mediator, partially explaining educational differences in BzRA use, regardless of mental health status.
Discussion: Work-related uncertainty leads to increased prescribing and medication use, regardless of mental health. Medicalisation and pharmaceuticalisation processes detach social problems from their social roots and treat them as personal failures. The marginalization of the social roots of unemployment, sick leave and involuntary (pre-)retirement has led to a personalization of responsibility. Negative feelings arising from such work statuses may cause isolated, non-specific symptoms for which medical treatment is sought.
Keywords: benzodiazepines; education; employment; health inequities; medicalization; mental health; psychotropic drugs.
Copyright © 2023 Colman, Delaruelle, Bracke and Ceuterick.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Benzodiazepine Use and Deprescribing in Belgian Nursing Homes: Results from the COME-ON Study.J Am Geriatr Soc. 2020 Dec;68(12):2768-2777. doi: 10.1111/jgs.16751. Epub 2020 Aug 12. J Am Geriatr Soc. 2020. PMID: 32786002 Clinical Trial.
-
Trends in benzodiazepine receptor agonists use and associated factors in the Belgian general older population: analysis of the Belgian health interview survey data.Ther Adv Psychopharmacol. 2021 May 25;11:20451253211011874. doi: 10.1177/20451253211011874. eCollection 2021. Ther Adv Psychopharmacol. 2021. PMID: 34104414 Free PMC article.
-
Association between employment status and risk of all-cause and cause-specific mortality: a population-based prospective cohort study.J Epidemiol Community Health. 2020 May;74(5):428-436. doi: 10.1136/jech-2019-213179. Epub 2020 Feb 21. J Epidemiol Community Health. 2020. PMID: 32086372
-
[What support of young presenting a first psychotic episode, when schooling is being challenged?].Encephale. 2017 Dec;43(6):570-576. doi: 10.1016/j.encep.2017.10.001. Epub 2017 Nov 8. Encephale. 2017. PMID: 29128195 Review. French.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
Cited by
-
Increased Risk of Sudden Sensorineural Hearing Loss in Patients Receiving Sedative-Hypnotics: A Propensity Score Weighting Cohort Study.Nat Sci Sleep. 2024 Dec 25;16:2231-2241. doi: 10.2147/NSS.S491544. eCollection 2024. Nat Sci Sleep. 2024. PMID: 39735386 Free PMC article.
References
-
- Kirby M, Denihan A, Bruce I, Radic A, Coakley D, Lawlor BA. Benzodiazepine use among the elderly in the community. Int J Geriatr Psychiatry. (1999) 14:280–4. - PubMed
-
- Barbee JG. Memory, benzodiazepines, and anxiety: integration of theoretical and clinical perspectives. J Clin Psychiatry. (1993) 54:86–101. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources