

Cardiac amyloidosis: state-of-the-art review
- PMID: 37397865
- PMCID: PMC10308177
- DOI: 10.26599/1671-5411.2023.05.006
Cardiac amyloidosis: state-of-the-art review
Abstract
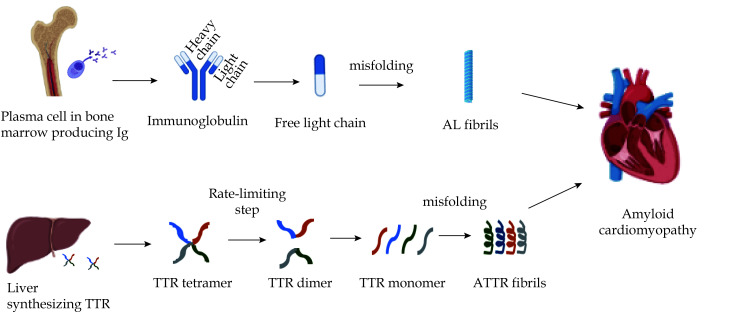
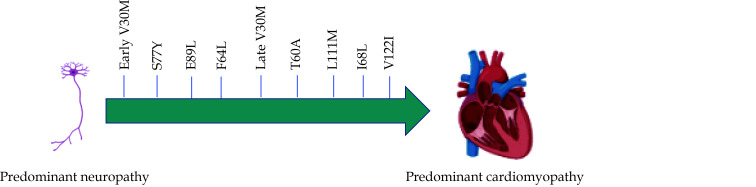
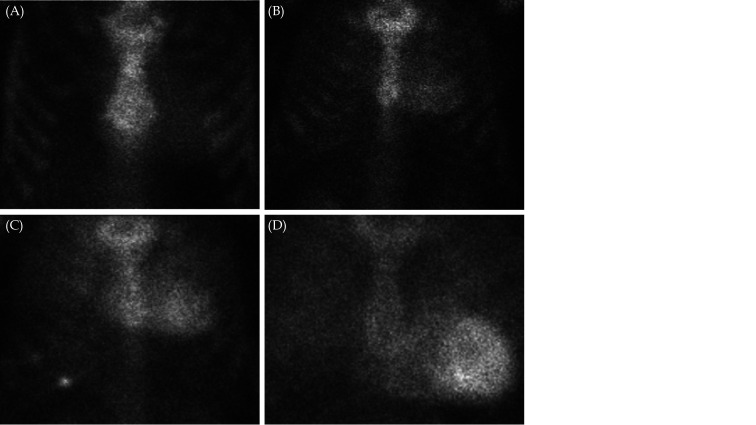
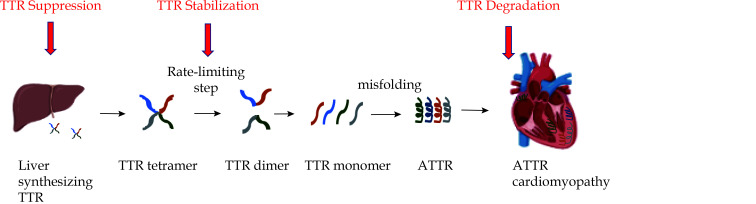
Cardiac amyloidosis (CA) is caused by deposition of amyloid fibrils in the myocardium and has two main subtypes, transthyretin cardiac amyloidosis (ATTR) and immunoglobulin light chain cardiac amyloidosis (AL). ATTR is further differentiated into wild-type (wtATTR) and hereditary (hATTR), depending on the absence or presence of mutation in the transthyretin gene. The increased recognition of disease with the improvement in diagnostic armamentarium and serendipitous advancements in the therapeutic landscape have changed the status of CA from being a rare and untreatable disease to being a not-so-rare and treatable disease. Both ATTR and AL have certain clinical aspects that can provide early clues for the disease. While electrocardiography followed by echocardiography and subsequently cardiac magnetic resonance can raise suspicion for CA, the definitive diagnosis of ATTR is non-invasively established by bone scintigraphy while that of AL always needs histological confirmation. Severity of CA can be gauged by serum biomarker-based staging of both ATTR and AL. ATTR therapies work by silencing or stabilizing TTR or by degrading amyloid fibrils, while AL is managed with anti-plasma cell therapies and autologous stem cell transplant.
© 2023 JGC All rights reserved; www.jgc301.com.
Figures

References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous