

This is a preprint.
Fetally-encoded GDF15 and maternal GDF15 sensitivity are major determinants of nausea and vomiting in human pregnancy
- PMID: 37398065
- PMCID: PMC10312505
- DOI: 10.1101/2023.06.02.542661
Fetally-encoded GDF15 and maternal GDF15 sensitivity are major determinants of nausea and vomiting in human pregnancy
Abstract
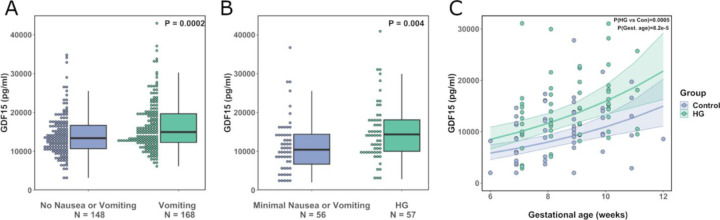
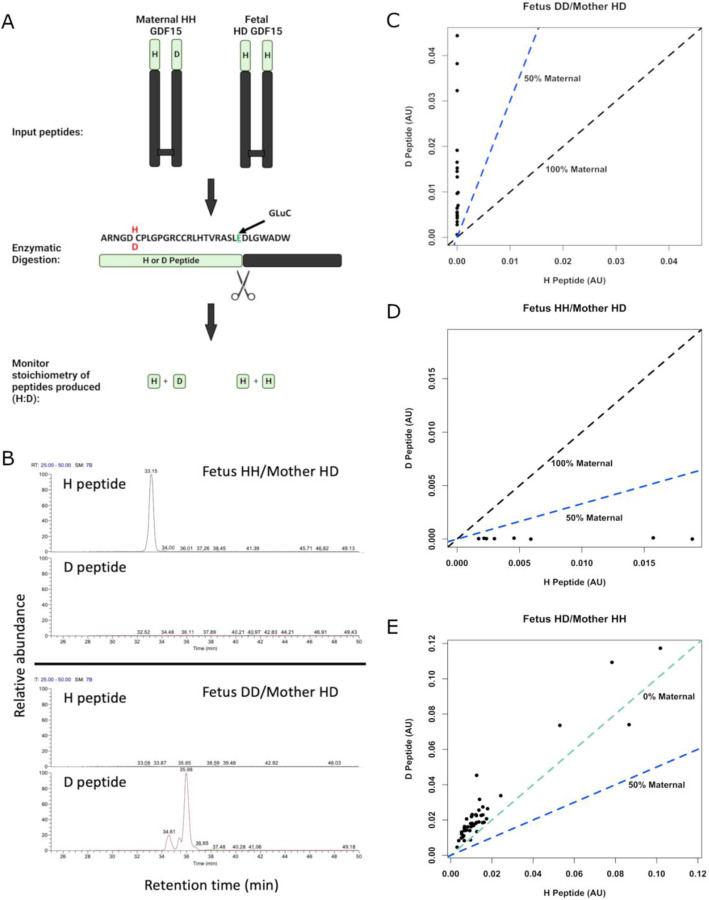
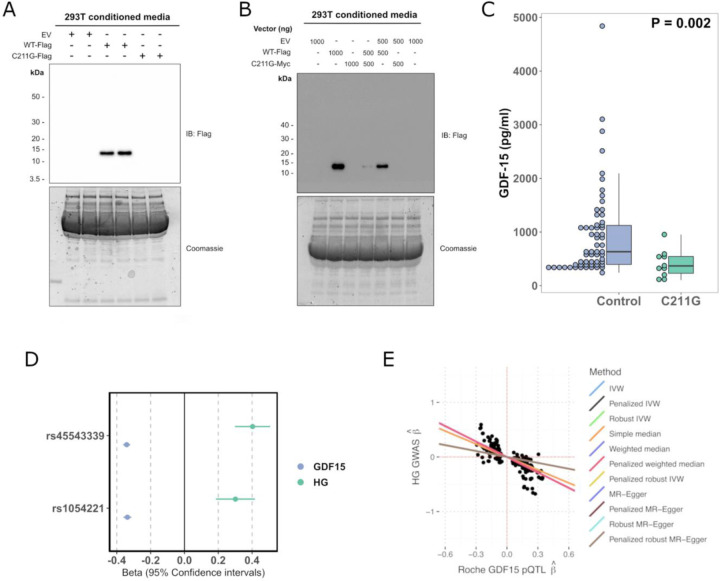
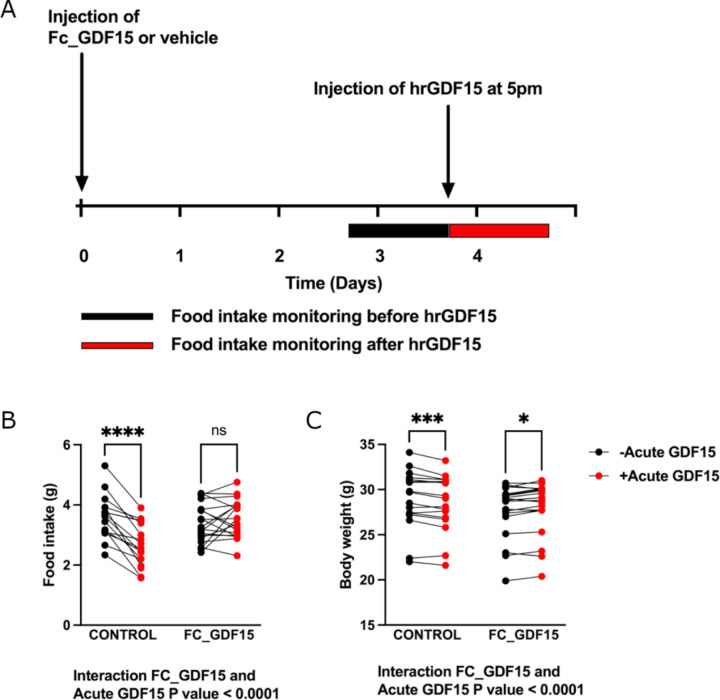
Human pregnancy is frequently accompanied by nausea and vomiting that may become severe and life-threatening, as in hyperemesis gravidarum (HG), the cause of which is unknown. Growth Differentiation Factor-15 (GDF15), a hormone known to act on the hindbrain to cause emesis, is highly expressed in the placenta and its levels in maternal blood rise rapidly in pregnancy. Variants in the maternal GDF15 gene are associated with HG. Here we report that fetal production of GDF15, and maternal sensitivity to it, both contribute substantially to the risk of HG. We found that the great majority of GDF15 in maternal circulation is derived from the feto-placental unit and that higher GDF15 levels in maternal blood are associated with vomiting and are further elevated in patients with HG. Conversely, we found that lower levels of GDF15 in the non-pregnant state predispose women to HG. A rare C211G variant in GDF15 which strongly predisposes mothers to HG, particularly when the fetus is wild-type, was found to markedly impair cellular secretion of GDF15 and associate with low circulating levels of GDF15 in the non-pregnant state. Consistent with this, two common GDF15 haplotypes which predispose to HG were associated with lower circulating levels outside pregnancy. The administration of a long-acting form of GDF15 to wild-type mice markedly reduced subsequent responses to an acute dose, establishing that desensitisation is a feature of this system. GDF15 levels are known to be highly and chronically elevated in patients with beta thalassemia. In women with this disorder, reports of symptoms of nausea or vomiting in pregnancy were strikingly diminished. Our findings support a causal role for fetal derived GDF15 in the nausea and vomiting of human pregnancy, with maternal sensitivity, at least partly determined by pre-pregnancy exposure to GDF15, being a major influence on its severity. They also suggest mechanism-based approaches to the treatment and prevention of HG.
Conflict of interest statement
Conflict of interest statement DSC-J reports non-financial support from Roche Diagnostics Ltd, outside the submitted work; G.C.S.S. reports personal fees and non-financial support from Roche Diagnostics Ltd, outside the submitted work; DSC-J and GCSS report grants from Sera Prognostics Inc, non-financial support from Illumina Inc, outside the submitted work. G.C.S.S. has been a paid consultant to GSK (preterm birth) and is a member of a Data Monitoring Committee for GSK trials of RSV vaccination in pregnancy. NS and PW has received grant funding from Roche diagnostics paid to their institution for biomarker work inclusive of GDF-15 measurements. JRBP is an employee and shareholder of Adrestia Therapeutics Ltd. KMG is a paid consultant for BYOMass Inc. CLM has received research funding and equipment at reduced cost from Dexcom Inc. GT is a full-time employee of Regeneron Genetics Center and receives salary, stock and stock options as compensation. FMG has received research grant support from Eli-Lilly and Astra Zeneca outside the scope of this current work. MSF is a paid consultant for Materna Biosciences, Inc. and a Board member and Science Advisor for the Hyperemesis Education and Research Foundation. SO has undertaken remunerated consultancy work for Pfizer, Third Rock Ventures, Astra Zeneca, NorthSea Therapeutics and Courage Therapeutics. NR, SML and SO are inventors/creators of a patent relating to this work.
Figures
References
-
- Fejzo M.S., et al., Nausea and vomiting of pregnancy and hyperemesis gravidarum. Nat Rev Dis Primers, 2019. 5(1): p. 62. - PubMed
-
- Gazmararian J.A., et al., Hospitalizations during pregnancy among managed care enrollees. Obstet Gynecol, 2002. 100(1): p. 94–100. - PubMed
-
- Breen D.M., et al., GDF-15 Neutralization Alleviates Platinum-Based Chemotherapy-Induced Emesis, Anorexia, and Weight Loss in Mice and Nonhuman Primates. Cell Metab, 2020. 32(6): p. 938–950.e6. - PubMed
-
- Moore A.G., et al., The transforming growth factor-ss superfamily cytokine macrophage inhibitory cytokine-1 is present in high concentrations in the serum of pregnant women. J Clin Endocrinol Metab, 2000. 85(12): p. 4781–8. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources