

This is a preprint.
Proposal of a new genomic framework for categorization of pediatric acute myeloid leukemia associated with prognosis
- PMID: 37398194
- PMCID: PMC10312943
- DOI: 10.21203/rs.3.rs-2925426/v1
Proposal of a new genomic framework for categorization of pediatric acute myeloid leukemia associated with prognosis
Update in
-
A new genomic framework to categorize pediatric acute myeloid leukemia.Nat Genet. 2024 Feb;56(2):281-293. doi: 10.1038/s41588-023-01640-3. Epub 2024 Jan 11. Nat Genet. 2024. PMID: 38212634 Free PMC article.
Abstract
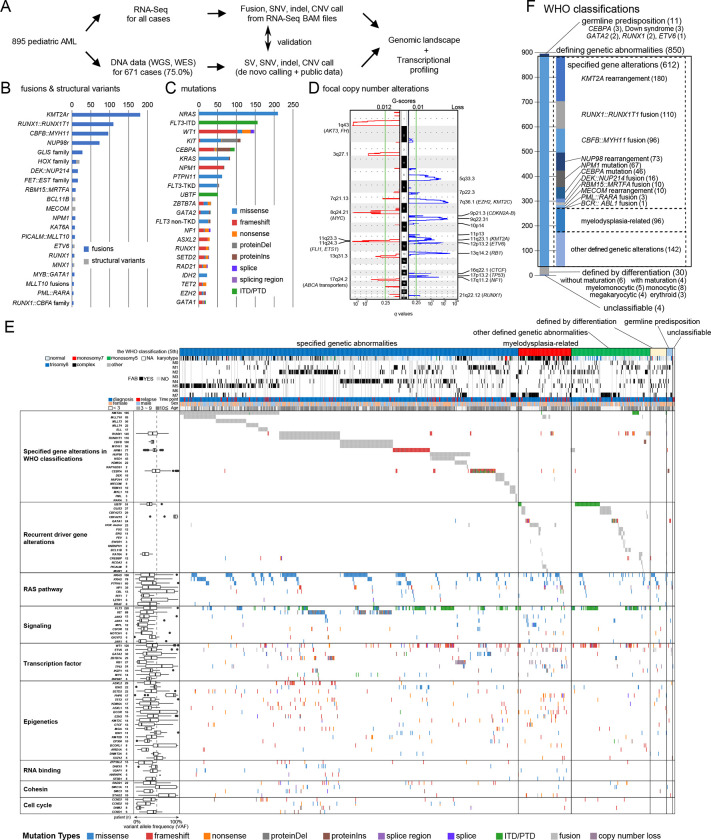
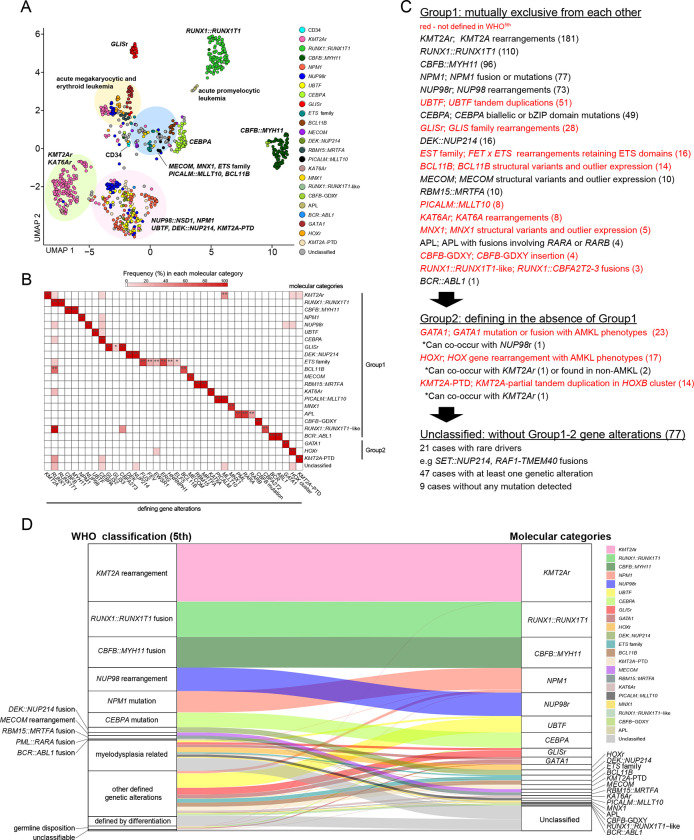
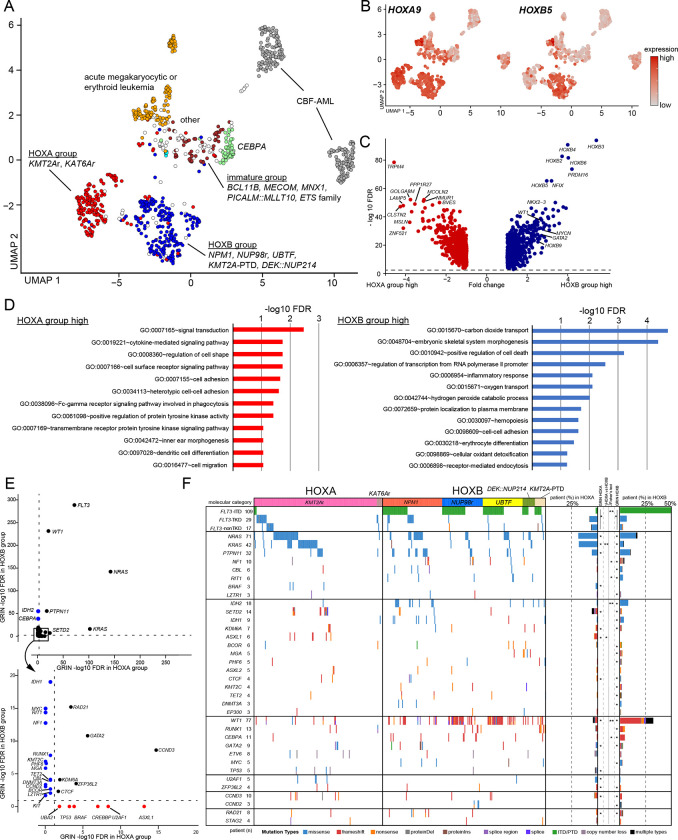
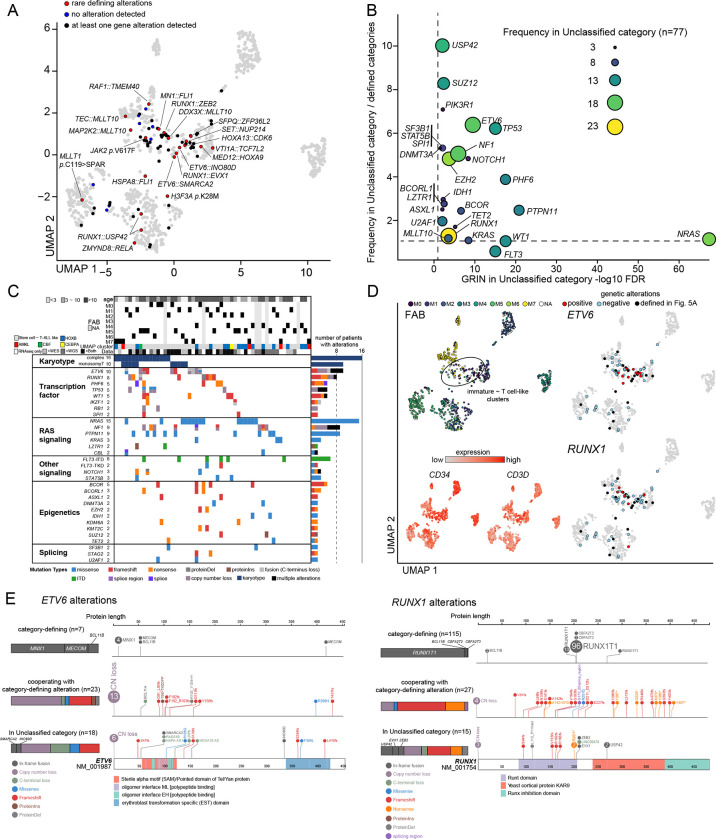
Recent studies on pediatric acute myeloid leukemia (pAML) have revealed pediatric-specific driver alterations, many of which are underrepresented in the current classification schemas. To comprehensively define the genomic landscape of pAML, we systematically categorized 895 pAML into 23 molecular categories that are mutually distinct from one another, including new entities such as UBTF or BCL11B, covering 91.4% of the cohort. These molecular categories were associated with unique expression profiles and mutational patterns. For instance, molecular categories characterized by specific HOXA or HOXB expression signatures showed distinct mutation patterns of RAS pathway genes, FLT3, or WT1, suggesting shared biological mechanisms. We show that molecular categories were strongly associated with clinical outcomes using two independent cohorts, leading to the establishment of a prognostic framework for pAML based on molecular categories and minimal residual disease. Together, this comprehensive diagnostic and prognostic framework forms the basis for future classification of pAML and treatment strategies.
Conflict of interest statement
Additional Declarations: There is NO Competing Interest.
Figures


References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
