

This is a preprint.
Supra-second interval timing in bipolar disorder: examining the role of disorder sub-type, mood, and medication status
- PMID: 37398216
- PMCID: PMC10312933
- DOI: 10.21203/rs.3.rs-3006203/v1
Supra-second interval timing in bipolar disorder: examining the role of disorder sub-type, mood, and medication status
Update in
-
Supra-second interval timing in bipolar disorder: examining the role of disorder sub-type, mood, and medication status.Int J Bipolar Disord. 2023 Oct 1;11(1):32. doi: 10.1186/s40345-023-00312-9. Int J Bipolar Disord. 2023. PMID: 37779127 Free PMC article.
Abstract
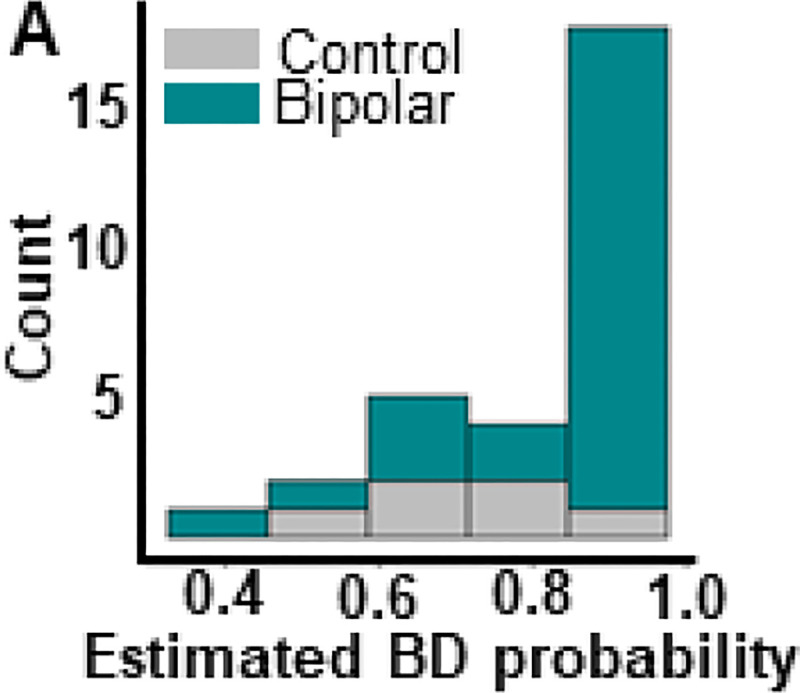
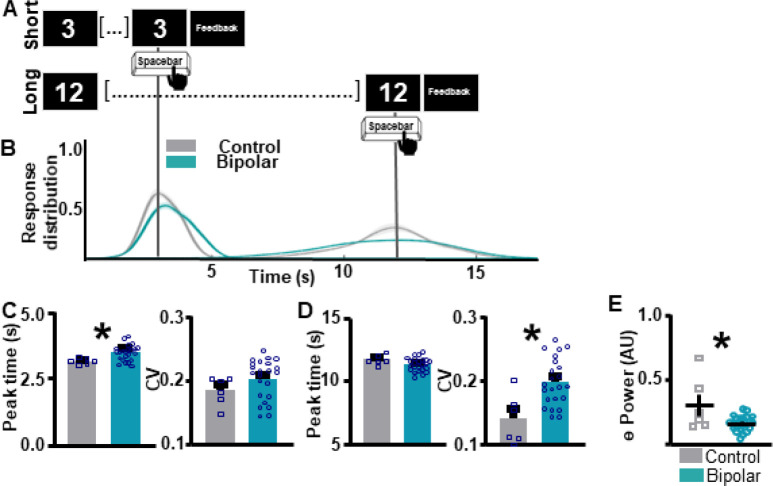
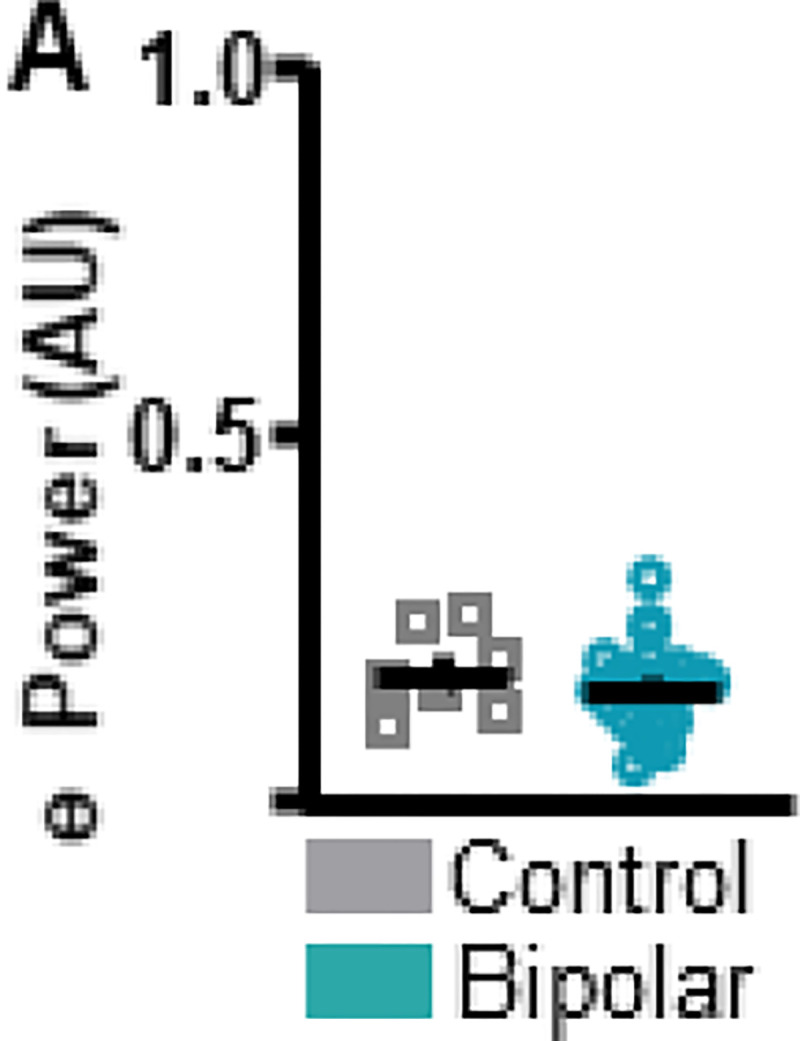
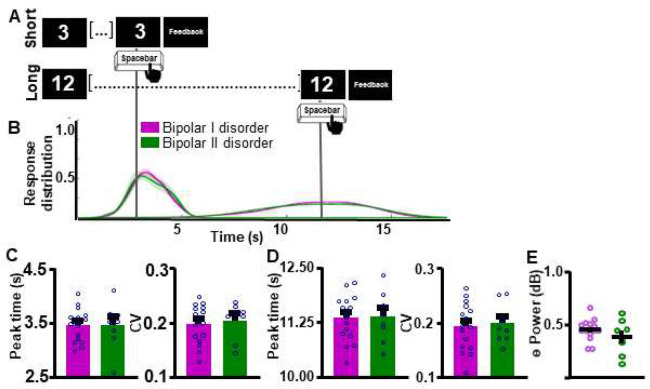
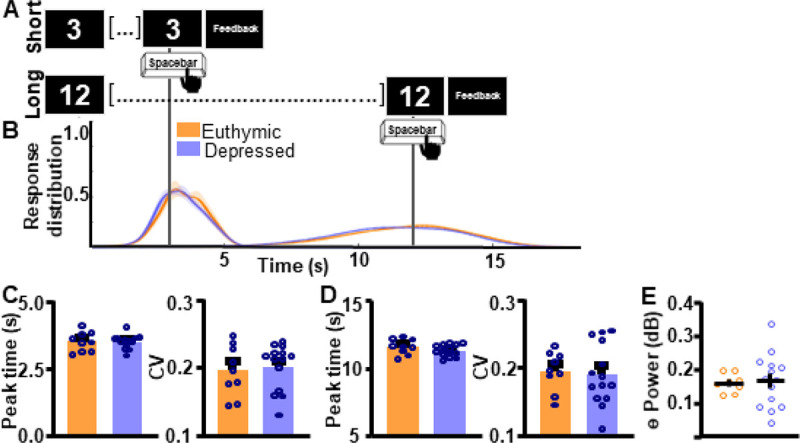
Background : Widely reported by bipolar disorder (BD) patients, cognitive symptoms, including deficits in executive function, memory, attention, and timing are under-studied. Work suggests that individuals with BD show impairments in interval timing tasks, including supra-second, sub-second, and implicit motor timing compared to the neuronormative population. However, how time perception differs within individuals with BD based on BD sub-type (BDI vs II), mood, or antipsychotic medication-use has not been thoroughly investigated. The present work administered a supra-second interval timing task concurrent with electroencephalography (EEG) to patients with BD and a neuronormative comparison group. As this task is known to elicit frontal theta oscillations, signal from the frontal (Fz) lead was analyzed at rest and during the task. Results : Results suggest that individuals with BD show impairments in supra-second interval timing and reduced frontal theta power compared during the task to neuronormative controls. However, within BD sub-groups, neither time perception nor frontal theta differed in accordance with BD sub-type, mood, or antipsychotic medication use. Conclusions : his work suggests that BD sub-type, mood status or antipsychotic medication use does not alter timing profile or frontal theta activity. Together with previous work, these findings point to timing impairments in BD patients across a wide range of modalities and durations indicating that an altered ability to assess the passage of time may be a fundamental cognitive abnormality in BD.
Conflict of interest statement
Competing interests:
The authors declare that they have no competing interests.
Figures

Similar articles
-
Supra-second interval timing in bipolar disorder: examining the role of disorder sub-type, mood, and medication status.Int J Bipolar Disord. 2023 Oct 1;11(1):32. doi: 10.1186/s40345-023-00312-9. Int J Bipolar Disord. 2023. PMID: 37779127 Free PMC article.
-
Cognitive deficits in bipolar disorders: Implications for emotion.Clin Psychol Rev. 2018 Feb;59:126-136. doi: 10.1016/j.cpr.2017.11.006. Epub 2017 Nov 21. Clin Psychol Rev. 2018. PMID: 29195773 Free PMC article. Review.
-
Internal clock variability, mood swings and working memory in bipolar disorder.J Affect Disord. 2022 Oct 15;315:48-56. doi: 10.1016/j.jad.2022.07.063. Epub 2022 Jul 27. J Affect Disord. 2022. PMID: 35907479
-
Resting-State Network Patterns Underlying Cognitive Function in Bipolar Disorder: A Graph Theoretical Analysis.Brain Connect. 2020 Sep;10(7):355-367. doi: 10.1089/brain.2019.0709. Epub 2020 Jul 21. Brain Connect. 2020. PMID: 32458698 Free PMC article.
-
Timing Tasks Synchronize Cerebellar and Frontal Ramping Activity and Theta Oscillations: Implications for Cerebellar Stimulation in Diseases of Impaired Cognition.Front Psychiatry. 2016 Jan 18;6:190. doi: 10.3389/fpsyt.2015.00190. eCollection 2015. Front Psychiatry. 2016. PMID: 26834650 Free PMC article. Review.
References
-
- Schaffer A, Isometsa ET, Tondo L, Moreno DH, Sinyor M, Kessing LV, et al. Epidemiology, neurobiology and pharmacological interventions related to suicide deaths and suicide attempts in bipolar disorder: Part I of a report of the International Society for Bipolar Disorders Task Force on Suicide in Bipolar Disorder. Aust N Z J Psychiatry. 2015;49(9):785–802. - PMC - PubMed
-
- Murray RM, Sham P, Van Os J, Zanelli J, Cannon M, McDonald C. A developmental model for similarities and dissimilarities between schizophrenia and bipolar disorder. Schizophr Res. 2004;71(2–3):405–16. - PubMed
-
- Zhou FC, Wang YY, Zheng W, Ungvari GS, Ng CH, Yuan Z, et al. Prospective memory in bipolar disorder: A meta-analysis. Psychiatry Res. 2018;259:184–90. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
