

This is a preprint.
Heterogeneous treatment effects of intensive glycemic control on kidney microvascular outcomes in ACCORD
- PMID: 37398349
- PMCID: PMC10312895
- DOI: 10.1101/2023.06.14.23291396
Heterogeneous treatment effects of intensive glycemic control on kidney microvascular outcomes in ACCORD
Update in
-
Heterogeneous Treatment Effects of Intensive Glycemic Control on Kidney Microvascular Outcomes and Mortality in ACCORD.J Am Soc Nephrol. 2024 Feb 1;35(2):216-228. doi: 10.1681/ASN.0000000000000272. Epub 2023 Dec 11. J Am Soc Nephrol. 2024. PMID: 38073026 Free PMC article.
Abstract
Objective: Clear criteria to individualize glycemic targets are lacking. In this post-hoc analysis of the Action to Control Cardiovascular Risk in Diabetes trial (ACCORD), we evaluate whether the kidney failure risk equation (KFRE) can identify patients who disproportionately benefit from intensive glycemic control on kidney microvascular outcomes.
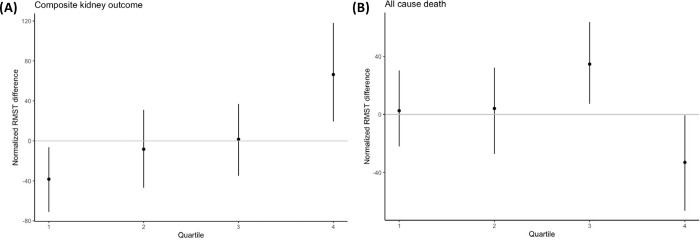
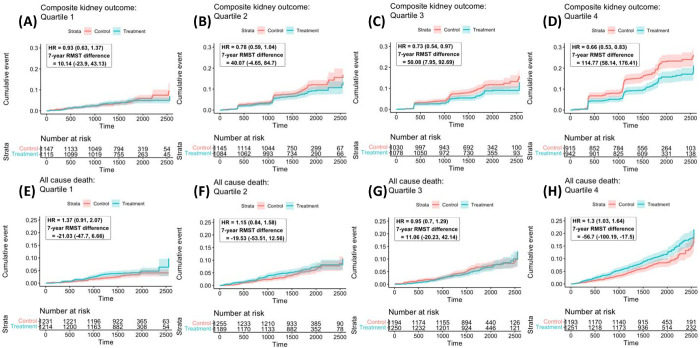
Research design and methods: We divided the ACCORD trial population in quartiles based on 5-year kidney failure risk using the KFRE. We estimated conditional treatment effects within each quartile and compared them to the average treatment effect in the trial. The treatment effects of interest were the 7-year restricted-mean-survival-time (RMST) differences between intensive and standard glycemic control arms on (1) time-to-first development of severely elevated albuminuria or kidney failure and (2) all-cause mortality.
Results: We found evidence that the effect of intensive glycemic control on kidney microvascular outcomes and all-cause mortality varies with baseline risk of kidney failure. Patients with elevated baseline risk of kidney failure benefitted the most from intensive glycemic control on kidney microvascular outcomes (7-year RMST difference of 115 v. 48 days in the entire trial population) However, this same patient group also experienced shorter times to death (7-year RMST difference of -57 v. -24 days).
Conclusions: We found evidence of heterogenous treatment effects of intensive glycemic control on kidney microvascular outcomes in ACCORD as a function of predicted baseline risk of kidney failure. Patients with higher kidney failure risk experienced the most pronounced benefits of treatment on kidney microvascular outcomes but also experienced the highest risk of all-cause mortality.
Conflict of interest statement
Conflicts of interest: The authors have no conflicts of interest to disclose.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources