

This is a preprint.
Single-tier point-of-care serodiagnosis of Lyme disease
- PMID: 37398357
- PMCID: PMC10312703
- DOI: 10.1101/2023.06.14.544508
Single-tier point-of-care serodiagnosis of Lyme disease
Update in
-
Rapid single-tier serodiagnosis of Lyme disease.Nat Commun. 2024 Aug 20;15(1):7124. doi: 10.1038/s41467-024-51067-5. Nat Commun. 2024. PMID: 39164226 Free PMC article.
Abstract
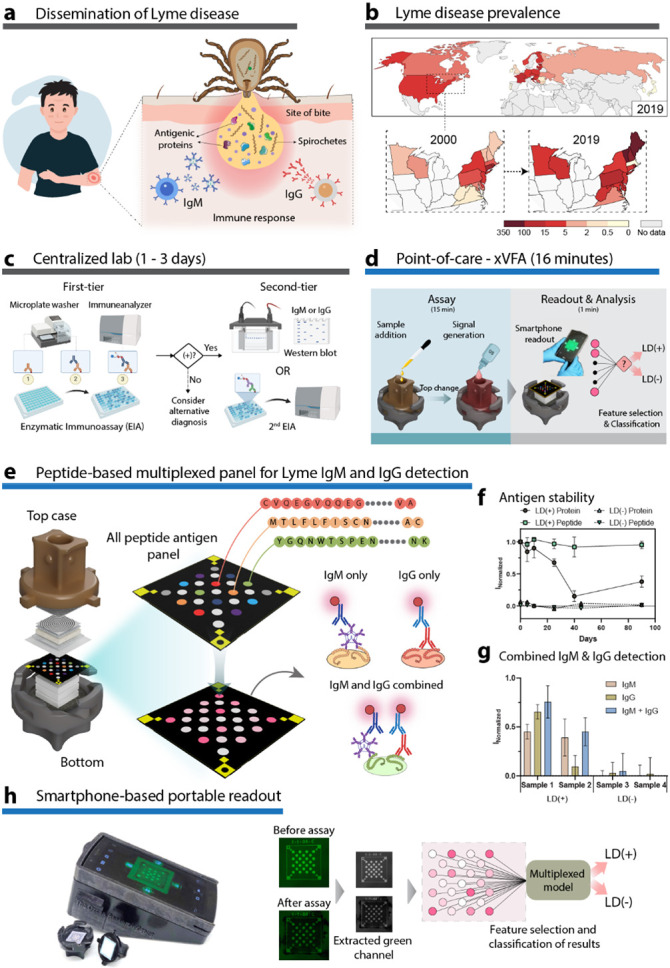
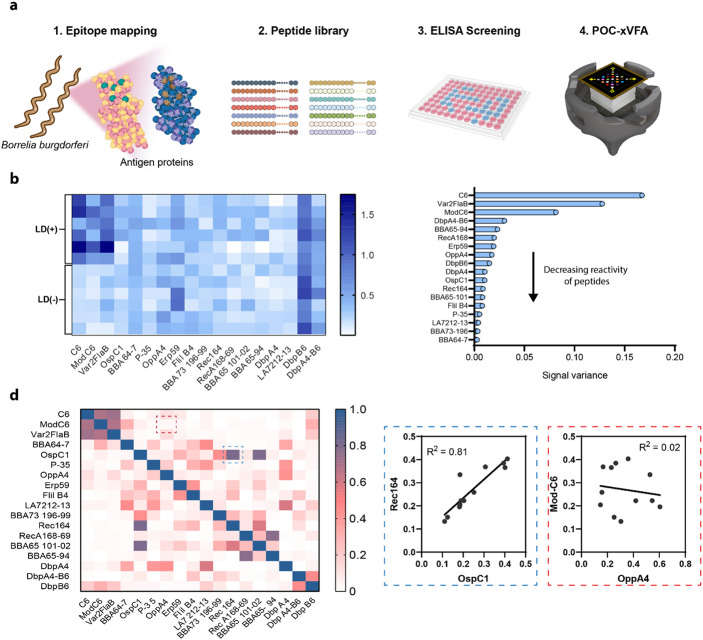
Point-of-care (POC) serological testing provides actionable information for several difficult to diagnose illnesses, empowering distributed health systems. Accessible and adaptable diagnostic platforms that can assay the repertoire of antibodies formed against pathogens are essential to drive early detection and improve patient outcomes. Here, we report a POC serologic test for Lyme disease (LD), leveraging synthetic peptides tuned to be highly specific to the LD antibody repertoire across patients and compatible with a paper-based platform for rapid, reliable, and cost-effective diagnosis. A subset of antigenic epitopes conserved across Borrelia burgdorferi genospecies and targeted by IgG and IgM antibodies, were selected based on their seroreactivity to develop a multiplexed panel for a single-step measurement of combined IgM and IgG antibodies from LD patient sera. Multiple peptide epitopes, when combined synergistically using a machine learning-based diagnostic model, yielded a high sensitivity without any loss in specificity. We blindly tested the platform with samples from the U.S. Centers for Disease Control & Prevention (CDC) LD repository and achieved a sensitivity and specificity matching the lab-based two-tier results with a single POC test, correctly discriminating cross-reactive look-alike diseases. This computational LD diagnostic test can potentially replace the cumbersome two-tier testing paradigm, improving diagnosis and enabling earlier effective treatment of LD patients while also facilitating immune monitoring and surveillance of the disease in the community.
Figures


References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous