

Policies and resources for strengthening of emergency and critical care services in the context of the global COVID-19 pandemic in Kenya
- PMID: 37399177
- PMCID: PMC10317215
- DOI: 10.1371/journal.pgph.0000483
Policies and resources for strengthening of emergency and critical care services in the context of the global COVID-19 pandemic in Kenya
Abstract
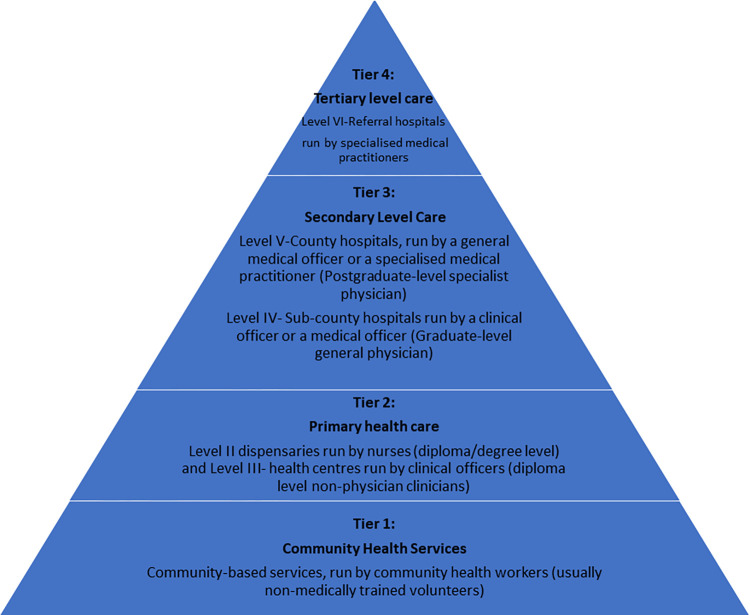
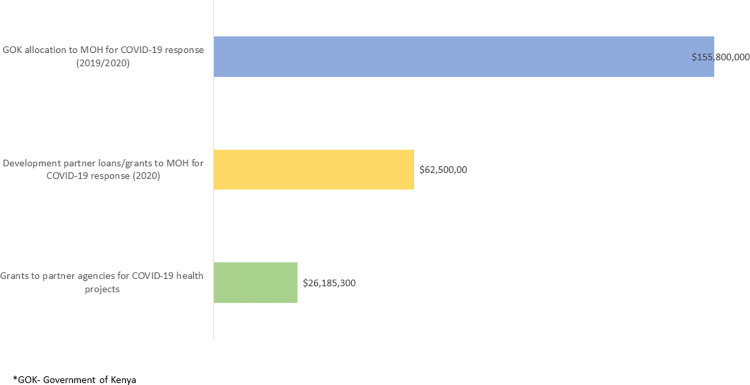
Critical illnesses cause several million deaths annually, with many of these occurring in low-resource settings like Kenya. Great efforts have been made worldwide to scale up critical care to reduce deaths from COVID-19. Lower income countries with fragile health systems may not have had sufficient resources to upscale their critical care. We aimed to review how efforts to strengthen emergency and critical care were operationalised during the pandemic in Kenya to point towards how future emergencies should be approached. This was an exploratory study that involved document reviews, and discussions with key stakeholders (donors, international agencies, professional associations, government actors), during the first year of the pandemic in Kenya. Our findings suggest that pre-pandemic health services for the critically ill in Kenya were sparse and unable to meet rising demand, with major limitations noted in human resources and infrastructure. The pandemic response saw galvanised action by the Government of Kenya and other agencies to mobilise resources (approximately USD 218 million). Earlier efforts were largely directed towards advanced critical care but since the human resource gap could not be reduced immediately, a lot of equipment remained unused. We also note that despite strong policies on what resources should be available, the reality on the ground was that there were often critical shortages. While emergency response mechanisms are not conducive to addressing long-term health system issues, the pandemic increased global recognition of the need to fund care for the critically ill. Limited resources may be best prioritised towards a public health approach with focus on provision of relatively basic, lower cost essential emergency and critical care (EECC) that can potentially save the most lives amongst critically ill patients.
Copyright: © 2023 Oliwa et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: TB: Technical consultancies with UNICEF, the World Bank, USAID and the Wellcome Trust, all outside the submitted work. ME: Financial competing interests – Grants from Wellcome and NIHR UK for research on hospital care in Kenya. Non-financial interest – Advisory roles for: WHO, Academy of Medical Sciences (UK), UKRI The other authors have no competing interests to declare. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Biccard BM, Gopalan PD, Miller M, Michell WL, Thomson D, Ademuyiwa A, et al.. Patient care and clinical outcomes for patients with COVID-19 infection admitted to African high-care or intensive care units (ACCCOS): a multicentre, prospective, observational cohort study. The Lancet. 2021;397(10288):1885–94. doi: 10.1016/S0140-6736(21)00441-4 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous