Identification of cuproptosis-related lncRNA for predicting prognosis and immunotherapeutic response in cervical cancer
- PMID: 37400520
- PMCID: PMC10318051
- DOI: 10.1038/s41598-023-37898-0
Identification of cuproptosis-related lncRNA for predicting prognosis and immunotherapeutic response in cervical cancer
Abstract
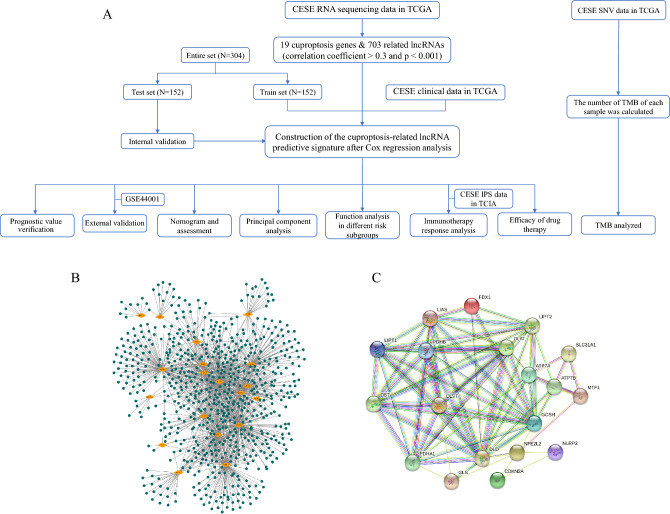
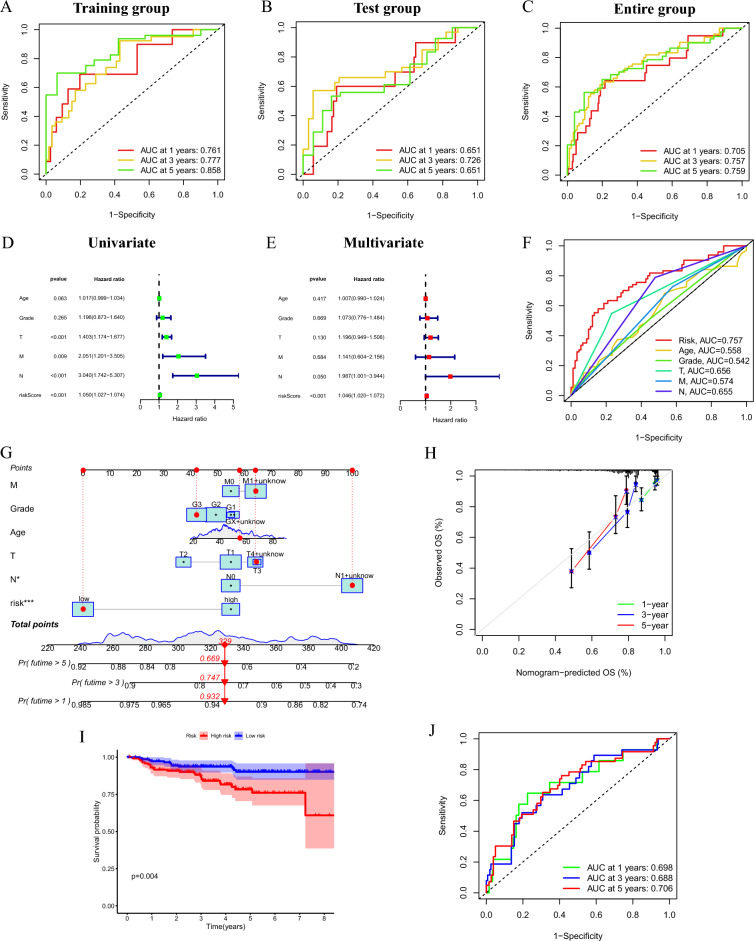
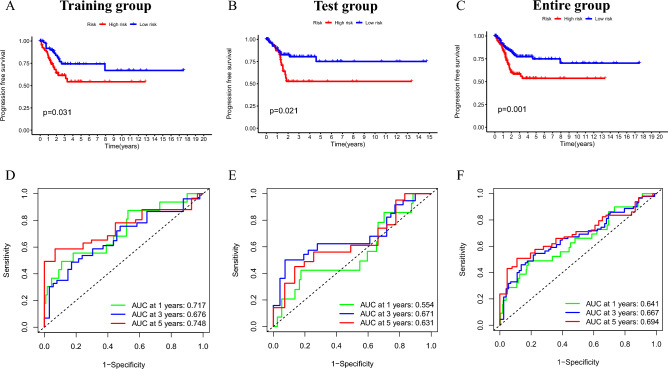
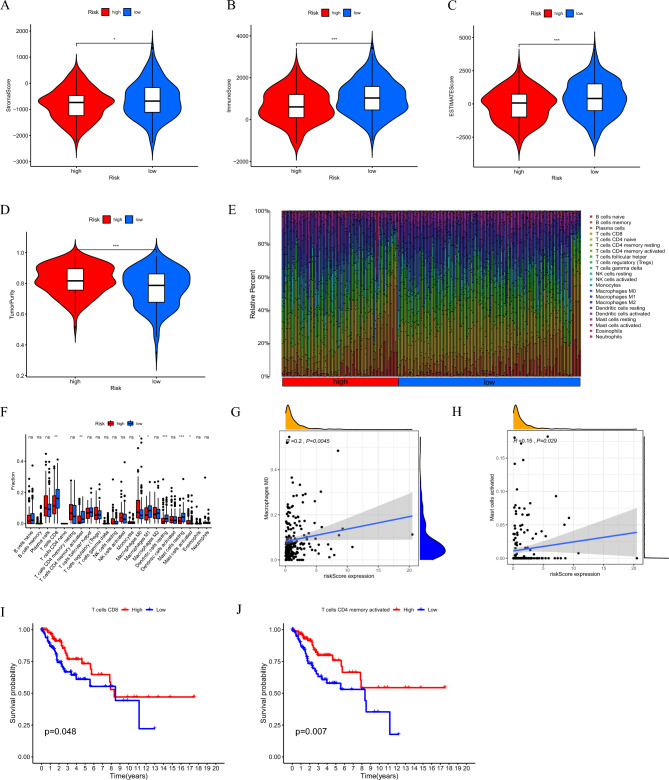
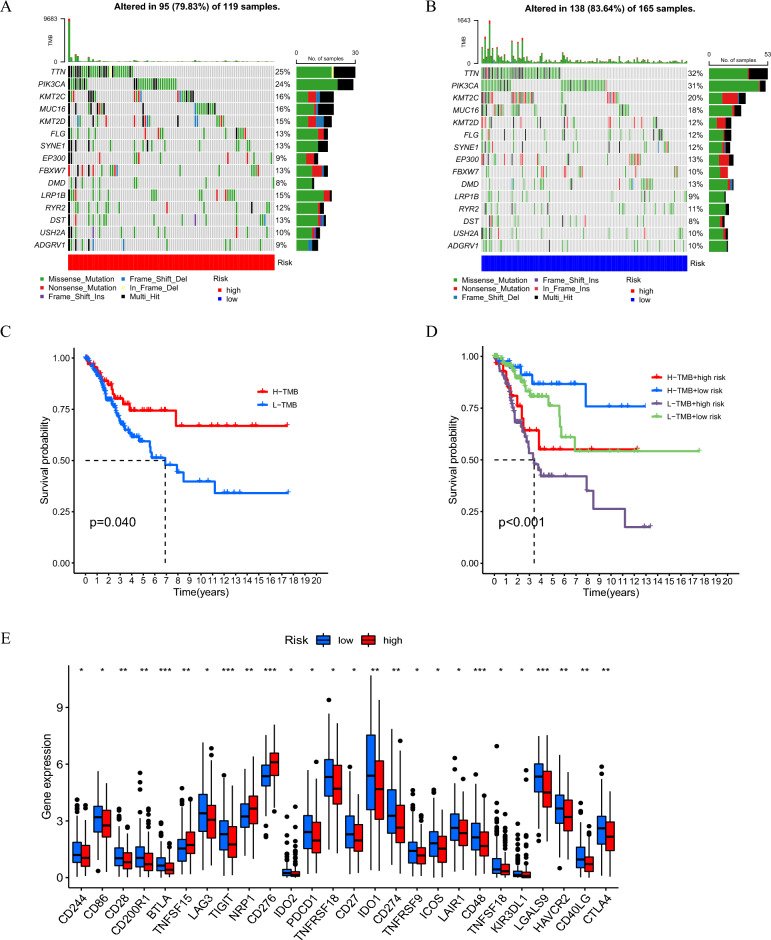
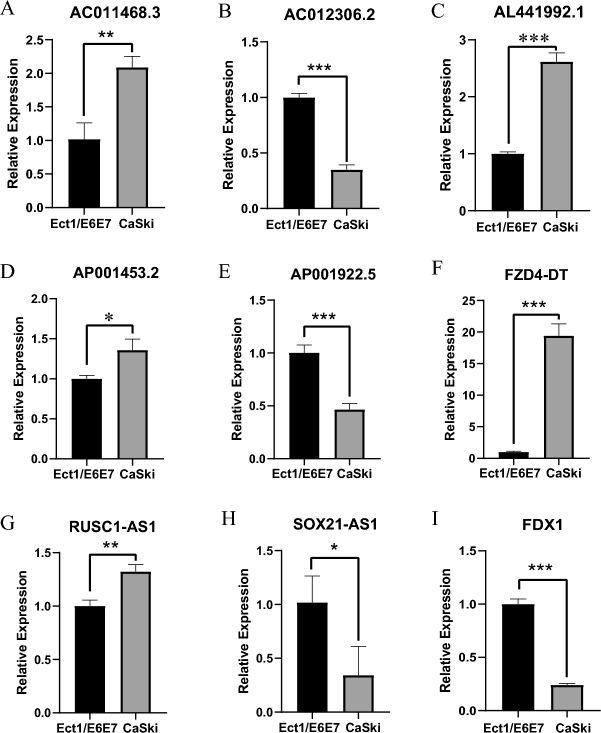
Patients diagnosed with advanced cervical cancer (CC) have poor prognosis after primary treatment, and there is a lack of biomarkers for predicting patients with an increased risk of recurrence of CC. Cuproptosis is reported to play a role in tumorigenesis and progression. However, the clinical impacts of cuproptosis-related lncRNAs (CRLs) in CC remain largely unclear. Our study attempted to identify new potential biomarkers to predict prognosis and response to immunotherapy with the aim of improving this situation. The transcriptome data, MAF files, and clinical information for CC cases were obtained from the cancer genome atlas, and Pearson correlation analysis was utilized to identify CRLs. In total, 304 eligible patients with CC were randomly assigned to training and test groups. LASSO regression and multivariate Cox regression were performed to construct a cervical cancer prognostic signature based on cuproptosis-related lncRNAs. Afterwards, we generated Kaplan-Meier curves, receiver operating characteristic curves and nomograms to verify the ability to predict prognosis of patients with CC. Genes for assessing differential expression among risk subgroups were also evaluated by functional enrichment analysis. Immune cell infiltration and the tumour mutation burden were analysed to explore the underlying mechanisms of the signature. Furthermore, the potential value of the prognostic signature to predict response to immunotherapy and sensitivity to chemotherapy drugs was examined. In our study, a risk signature containing eight cuproptosis-related lncRNAs (AL441992.1, SOX21-AS1, AC011468.3, AC012306.2, FZD4-DT, AP001922.5, RUSC1-AS1, AP001453.2) to predict the survival outcome of CC patients was developed, and the reliability of the risk signature was appraised. Cox regression analyses indicated that the comprehensive risk score is an independent prognostic factor. Moreover, significant differences were found in progression-free survival, immune cell infiltration, therapeutic response to immune checkpoint inhibitors, and IC50 for chemotherapeutic agents between risk subgroups, suggesting that our model can be well employed to assess the clinical efficacy of immunotherapy and chemotherapy. Based on our 8-CRLs risk signature, we were able to independently assess the outcome and response to immunotherapy of CC patients, and this signature might benefit clinical decision-making for individualized treatment.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures