

The Role and Clinical Outcomes of Endoscopic Spine Surgery of Treating Spinal Metastases; Outcomes of 29 Cases From 8 Countries
- PMID: 37401080
- PMCID: PMC10323327
- DOI: 10.14245/ns.2346274.137
The Role and Clinical Outcomes of Endoscopic Spine Surgery of Treating Spinal Metastases; Outcomes of 29 Cases From 8 Countries
Abstract
Objective: We aim to report the outcomes and feasibility of endoscopic spine surgery used to treat symptomatic spinal metastases patients. This is the most extensive series of spinal metastases patients who underwent endoscopic spine surgery.
Methods: A worldwide collaborative network group of endoscopic spine surgeons, named 'ESSSORG,' was established. Patients diagnosed with spinal metastases who underwent endoscopic spine surgery from 2012 to 2022 were retrospectively reviewed. All related patient data and clinical outcomes were gathered and analyzed before the surgery and the followtime period of 2 weeks, 1 month, 3 months, and 6 months.
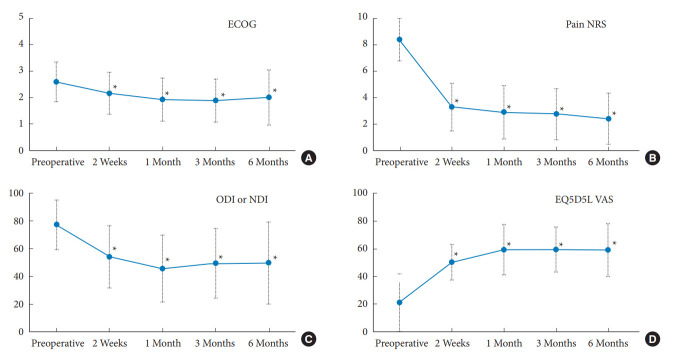
Results: A total of 29 patients from South Korea, Thailand, Taiwan, Mexico, Brazil, Argentina, Chile, and India, were included. The mean age was 59.59 years, and 11 of them were female. The total number of decompressed levels was 40. The technique was relatively equal (15 uniportal; 14 biportal). The average length of admission was 4.41 days. Of all patients with an American Spinal Injury Association Impairment Scale of D or lower before surgery, 62.06% reported having at least one recovery grade after the surgery. Almost all clinical outcomes parameters statistically significantly improved and maintained from 2 weeks to 6 months after the surgery. Few surgical-related complications (4 cases) were reported.
Conclusion: Endoscopic spine surgery is a valid option for treating spinal metastases patients as it could yield comparable results to other minimally invasive spine surgery techniques. As the aim is to improve the quality of life, this procedure is valuable and holds value in palliative oncologic spine surgery.
Keywords: Endoscopic spine surgery; Minimally invasive spine surgery; Palliative surgery; Quality of life; Spinal metastases.
Conflict of interest statement
The corresponding author (JSK) is a consultant of Richard Wolf, GmbH, and Elliquence, LLC. The other authors have no conflicts of interest to declare.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
