Transepidermal water loss rises before food anaphylaxis and predicts food challenge outcomes
- PMID: 37402149
- PMCID: PMC10425212
- DOI: 10.1172/JCI168965
Transepidermal water loss rises before food anaphylaxis and predicts food challenge outcomes
Abstract
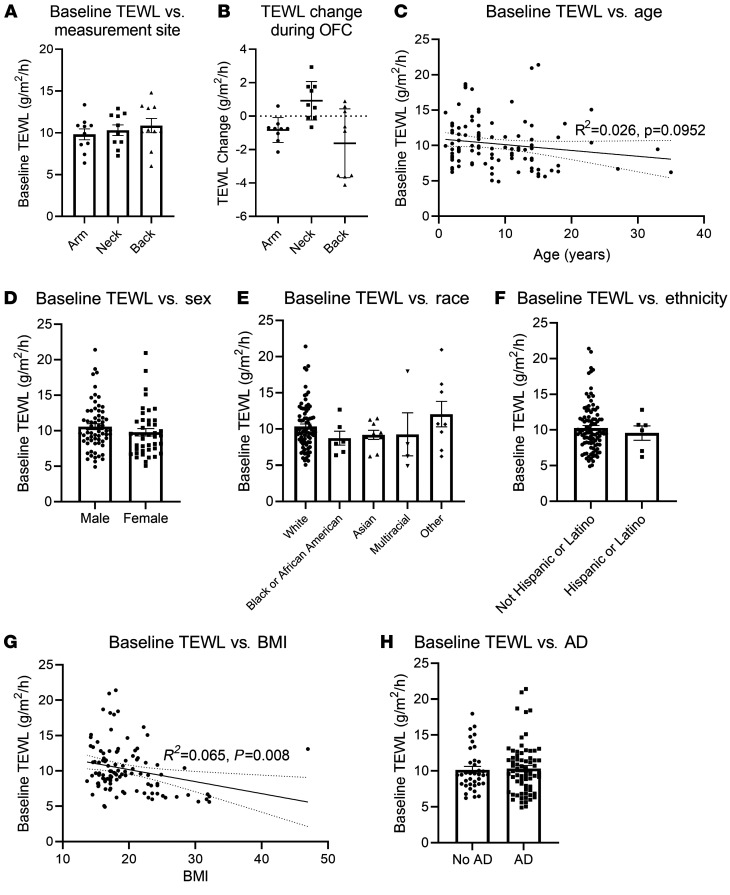
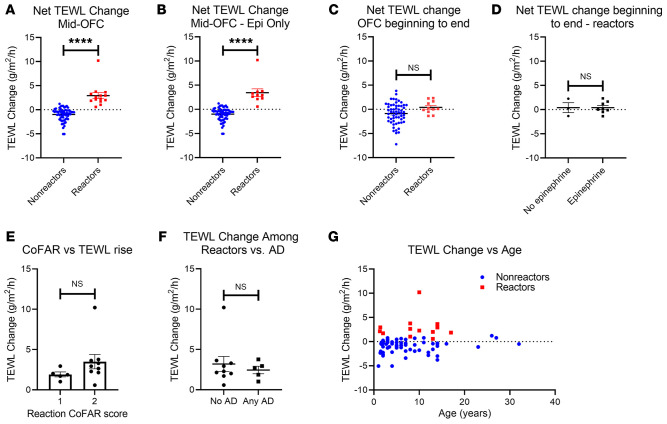
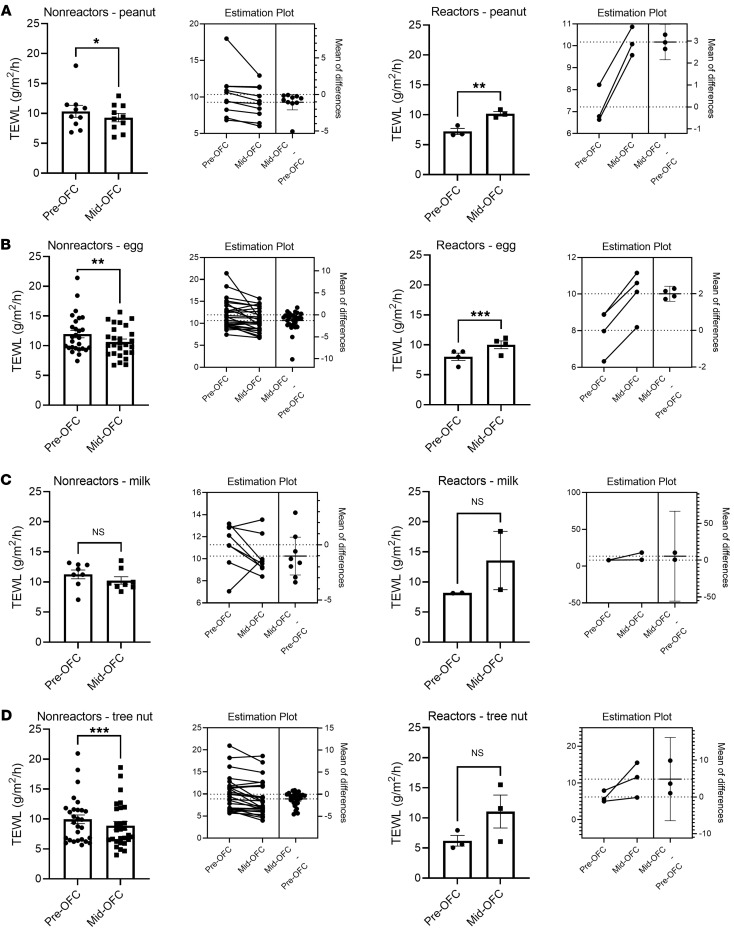
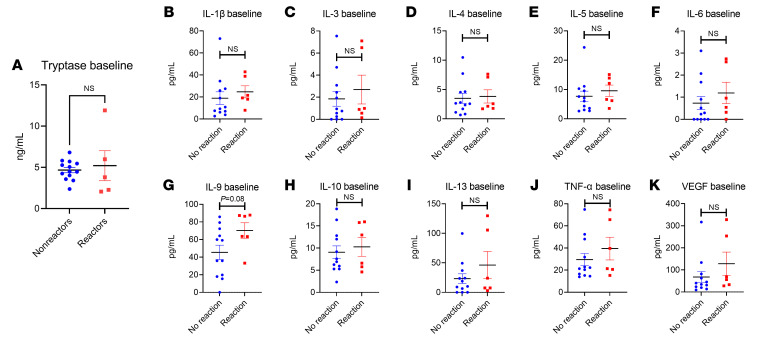
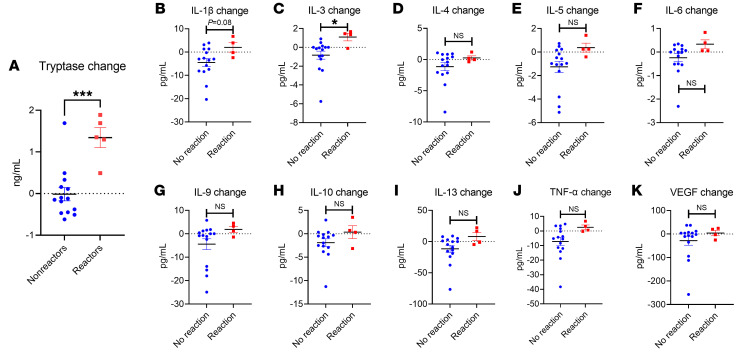
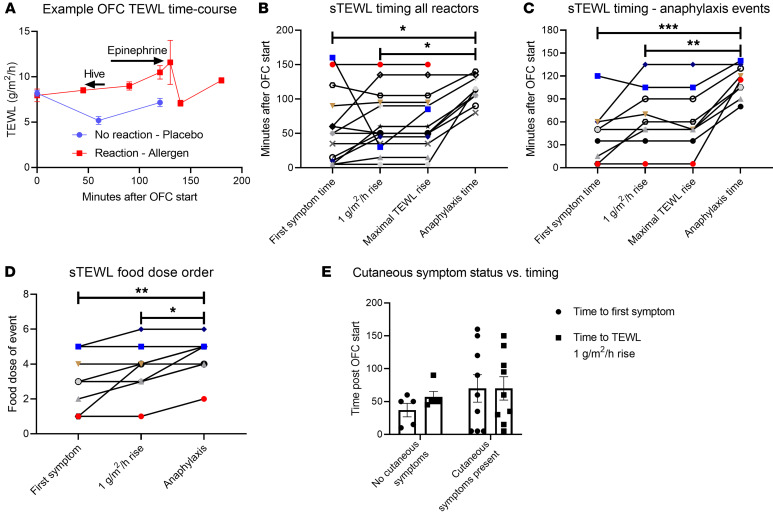
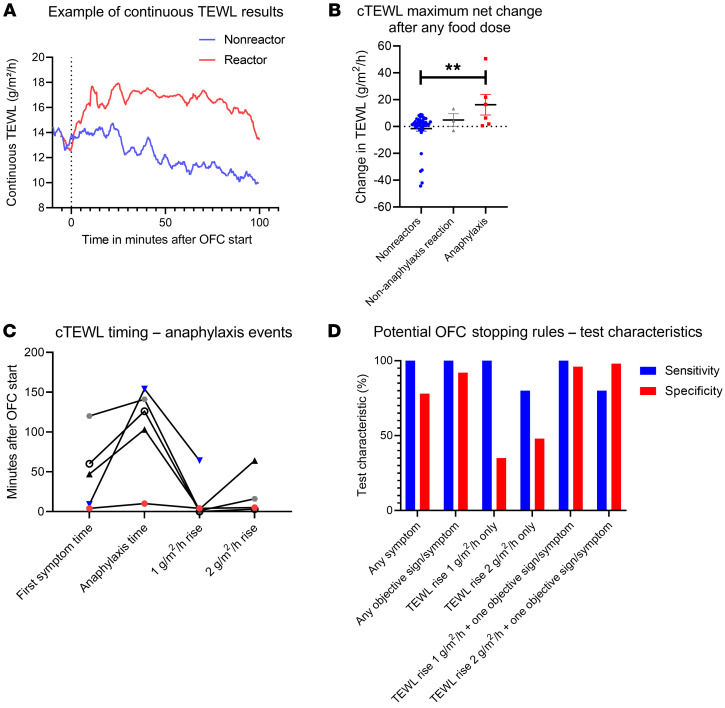
BACKGROUNDFood allergy (FA) is a growing health problem requiring physiologic confirmation via the oral food challenge (OFC). Many OFCs result in clinical anaphylaxis, causing discomfort and risk while limiting OFC utility. Transepidermal water loss (TEWL) measurement provides a potential solution to detect food anaphylaxis in real time prior to clinical symptoms. We evaluated whether TEWL changes during an OFC could predict anaphylaxis onset.METHODSPhysicians and nurses blinded to the TEWL results conducted and adjudicated the results of all 209 OFCs in this study. A study coordinator measured TEWL throughout the OFC and had no input on the OFC conduct. TEWL was measured 2 ways in 2 separate groups. First, TEWL was measured using static, discrete measurements. Second, TEWL was measured using continuous monitoring. Participants who consented provided blood samples before and after the OFCs for biomarker analyses.RESULTSTEWL rose significantly (2.93 g/m2/h) during reactions and did not rise during nonreacting OFCs (-1.00 g/m2/h). Systemic increases in tryptase and IL-3 were also detected during reactions, providing supporting biochemical evidence of anaphylaxis. The TEWL rise occurred 48 minutes earlier than clinically evident anaphylaxis. Continuous monitoring detected a significant rise in TEWL that presaged positive OFCs, but no rise was seen in the OFCs that resulted in no reaction, providing high predictive specificity (96%) for anaphylaxis against nonreactions 38 minutes prior to anaphylaxis onset.CONCLUSIONSDuring OFCs, a TEWL rise anticipated a positive clinical challenge. TEWL presents a monitoring modality that may predict food anaphylaxis and facilitate improvements in OFC safety and tolerability.
Keywords: Allergy; Clinical practice; Diagnostics; Immunology; Inflammation.
Figures