

Evaluation of medication regimen complexity as a predictor for mortality
- PMID: 37402869
- PMCID: PMC10319715
- DOI: 10.1038/s41598-023-37908-1
Evaluation of medication regimen complexity as a predictor for mortality
Abstract
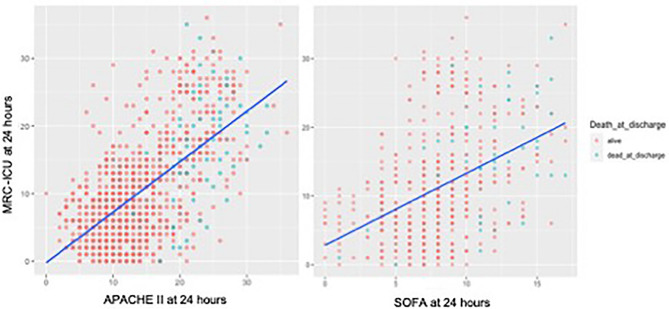
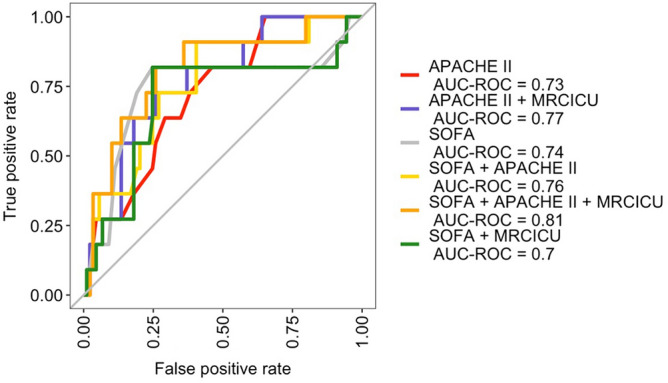
While medication regimen complexity, as measured by a novel medication regimen complexity-intensive care unit (MRC-ICU) score, correlates with baseline severity of illness and mortality, whether the MRC-ICU improves hospital mortality prediction is not known. After characterizing the association between MRC-ICU, severity of illness and hospital mortality we sought to evaluate the incremental benefit of adding MRC-ICU to illness severity-based hospital mortality prediction models. This was a single-center, observational cohort study of adult intensive care units (ICUs). A random sample of 991 adults admitted ≥ 24 h to the ICU from 10/2015 to 10/2020 were included. The logistic regression models for the primary outcome of mortality were assessed via area under the receiver operating characteristic (AUROC). Medication regimen complexity was evaluated daily using the MRC-ICU. This previously validated index is a weighted summation of medications prescribed in the first 24 h of ICU stay [e.g., a patient prescribed insulin (1 point) and vancomycin (3 points) has a MRC-ICU = 4 points]. Baseline demographic features (e.g., age, sex, ICU type) were collected and severity of illness (based on worst values within the first 24 h of ICU admission) was characterized using both the Acute Physiology and Chronic Health Evaluation (APACHE II) and the Sequential Organ Failure Assessment (SOFA) score. Univariate analysis of 991 patients revealed every one-point increase in the average 24-h MRC-ICU score was associated with a 5% increase in hospital mortality [Odds Ratio (OR) 1.05, 95% confidence interval 1.02-1.08, p = 0.002]. The model including MRC-ICU, APACHE II and SOFA had a AUROC for mortality of 0.81 whereas the model including only APACHE-II and SOFA had a AUROC for mortality of 0.76. Medication regimen complexity is associated with increased hospital mortality. A prediction model including medication regimen complexity only modestly improves hospital mortality prediction.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
