

The Evolving Treatment Landscape of Merkel Cell Carcinoma
- PMID: 37403007
- PMCID: PMC11260505
- DOI: 10.1007/s11864-023-01118-8
The Evolving Treatment Landscape of Merkel Cell Carcinoma
Abstract
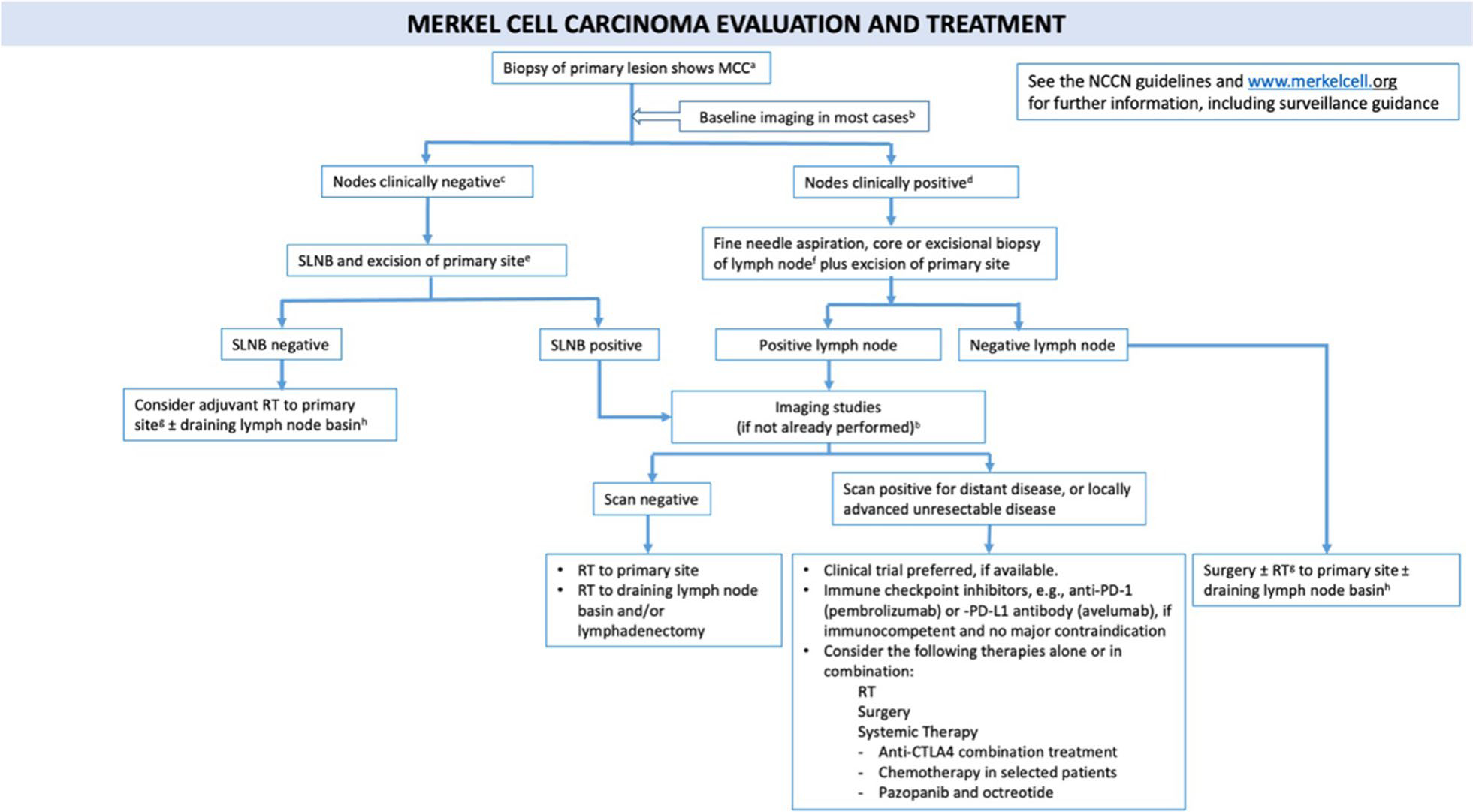
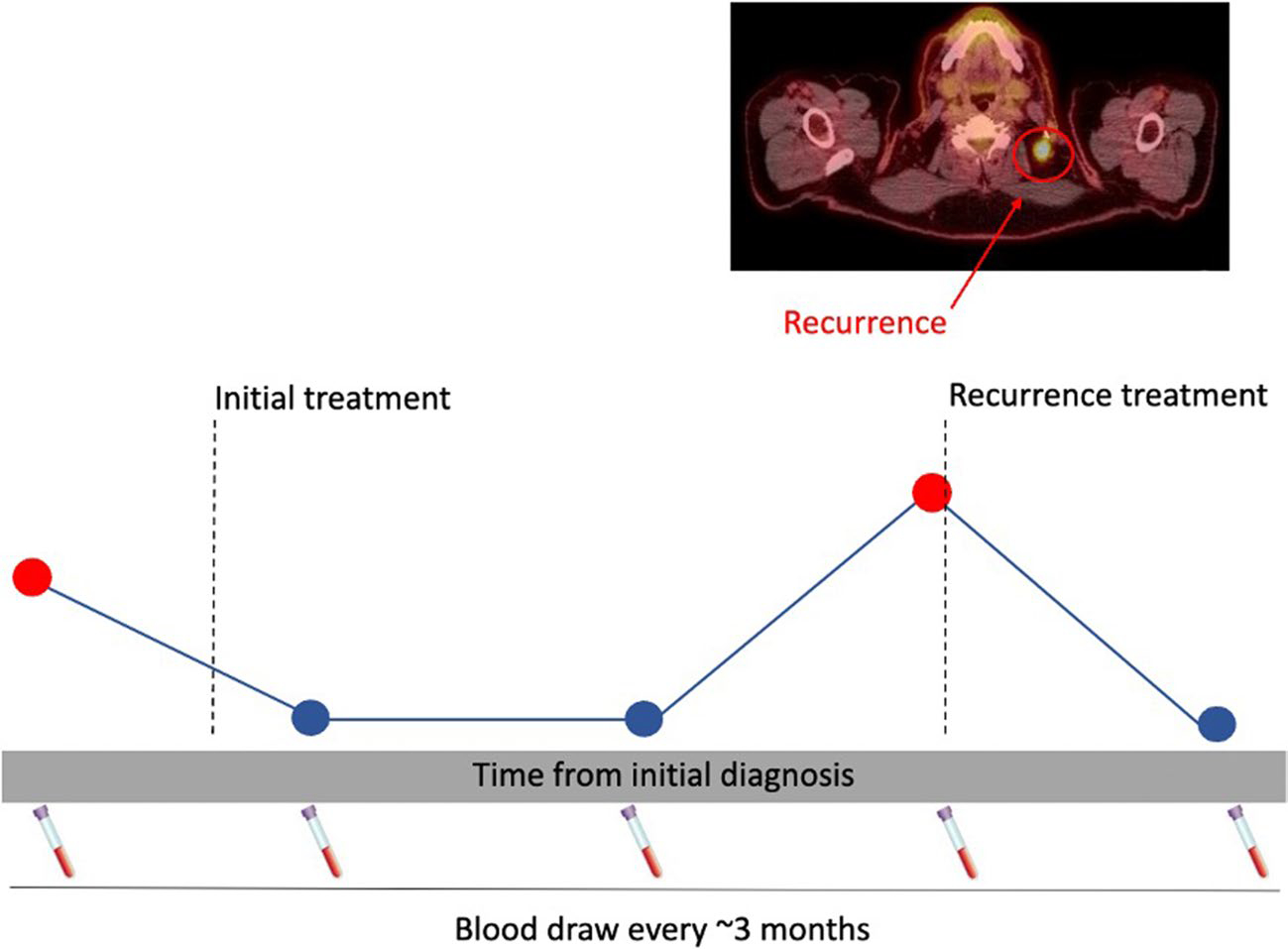
Merkel cell carcinoma (MCC) has a high risk of recurrence and requires unique treatment relative to other skin cancers. The patient population is generally older, with comorbidities. Multidisciplinary and personalized care is therefore paramount, based on patient preferences regarding risks and benefits. Positron emission tomography and computed tomography (PET-CT) is the most sensitive staging modality and reveals clinically occult disease in ~ 16% of patients. Discovery of occult disease spread markedly alters management. Newly diagnosed, localized disease is often managed with sentinel lymph node biopsy (SLNB), local excision, primary wound closure, and post-operative radiation therapy (PORT). In contrast, metastatic disease is usually treated systemically with an immune checkpoint inhibitor (ICI). However, one or more of these approaches may not be indicated. Criteria for such exceptions and alternative approaches will be discussed. Because MCC recurs in 40% of patients and early detection/treatment of advanced disease is advantageous, close surveillance is recommended. Given that over 90% of initial recurrences arise within 3 years, surveillance frequency can be rapidly decreased after this high-risk period. Patient-specific assessment of risk is important because recurrence risk varies widely (15 to > 80%: Merkelcell.org/recur) depending on baseline patient characteristics and time since treatment. Blood-based surveillance tests are now available (Merkel cell polyomavirus (MCPyV) antibodies and circulating tumor DNA (ctDNA)) with excellent sensitivity that can spare patients from contrast dye, radioactivity, and travel to a cancer imaging facility. If recurrent disease is locoregional, management with surgery and/or RT is typically indicated. ICIs are now the first line for systemic/advanced MCC, with objective response rates (ORRs) exceeding 50%. Cytotoxic chemotherapy is sometimes used for debulking disease or in patients who cannot tolerate ICI. ICI-refractory disease is the major problem faced by this field. Fortunately, numerous promising therapies are on the horizon to address this clinical need.
Keywords: Cutaneous neuroendocrine carcinoma; Immunotherapy; Merkel cell carcinoma; Merkel cell polyomavirus; Multidisciplinary care.
© 2023. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Compliance with Ethical Standards
Conflict of Interest
Paul Nghiem has served as a consultant for: EMD Serono, Merck, and Pfizer/Regeneron; his institution has received research funding from Bristol-Myers Squibb and EMD Serono. Neha Singh, Erin McClure, Peter Goff, Emily Huynh, Song Park, and Tomoko Akaike declare no conflicts of interest with this work.
Figures

Similar articles
-
Merkel Cell Carcinoma of Unknown Primary Origin.Acta Dermatovenerol Croat. 2023 Dec;31(3):153-155. Acta Dermatovenerol Croat. 2023. PMID: 38439727
-
Scientific and clinical developments in Merkel cell carcinoma: A polyomavirus-driven, often-lethal skin cancer.J Dermatol Sci. 2022 Jan;105(1):2-10. doi: 10.1016/j.jdermsci.2021.10.004. Epub 2021 Oct 18. J Dermatol Sci. 2022. PMID: 34836718 Free PMC article. Review.
-
Merkel Cell Carcinoma Therapeutic Update.Curr Treat Options Oncol. 2016 Jul;17(7):36. doi: 10.1007/s11864-016-0409-1. Curr Treat Options Oncol. 2016. PMID: 27262710 Free PMC article. Review.
-
Clinical benefit of baseline imaging in Merkel cell carcinoma: Analysis of 584 patients.J Am Acad Dermatol. 2021 Feb;84(2):330-339. doi: 10.1016/j.jaad.2020.07.065. Epub 2020 Jul 21. J Am Acad Dermatol. 2021. PMID: 32707254 Free PMC article.
-
Diagnosis and treatment of Merkel cell carcinoma: European consensus-based interdisciplinary guideline - Update 2022.Eur J Cancer. 2022 Aug;171:203-231. doi: 10.1016/j.ejca.2022.03.043. Epub 2022 Jun 19. Eur J Cancer. 2022. PMID: 35732101 Review.
Cited by
-
IMPDH inhibition induces DNA replication stress and ATR sensitivity in Merkel cell carcinoma.iScience. 2025 May 2;28(6):112567. doi: 10.1016/j.isci.2025.112567. eCollection 2025 Jun 20. iScience. 2025. PMID: 40491496 Free PMC article.
-
Predictive and Interpretable Machine Learning of Economic Burden: The Role of Chronic Conditions Among Elderly Patients with Incident Primary Merkel Cell Carcinoma (MCC).Clinicoecon Outcomes Res. 2024 Dec 11;16:847-868. doi: 10.2147/CEOR.S456968. eCollection 2024. Clinicoecon Outcomes Res. 2024. PMID: 39678935 Free PMC article.
-
A Rapidly Developing Nodule in a Patient With Hairy Cell Leukemia in Remission: Merkel Cell Carcinoma: A Case Report.In Vivo. 2024 Sep-Oct;38(5):2540-2544. doi: 10.21873/invivo.13727. In Vivo. 2024. PMID: 39187345 Free PMC article.
-
Development of a Multiplex Immunofluorescence Assay for Tumor Microenvironment Studies of Human and Murine Merkel Cell Carcinoma.Lab Invest. 2024 Oct;104(10):102128. doi: 10.1016/j.labinv.2024.102128. Epub 2024 Aug 23. Lab Invest. 2024. PMID: 39182611
-
Merkel cell carcinoma: updates in tumor biology, emerging therapies, and preclinical models.Front Oncol. 2024 Jul 29;14:1413793. doi: 10.3389/fonc.2024.1413793. eCollection 2024. Front Oncol. 2024. PMID: 39136002 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
