

Impact of flail chest injury on morbidity and outcome: ten years' experience at a tertiary care hospital in a developing country
- PMID: 37403012
- PMCID: PMC10318665
- DOI: 10.1186/s12871-023-02185-y
Impact of flail chest injury on morbidity and outcome: ten years' experience at a tertiary care hospital in a developing country
Abstract
Background: One of the worst types of severe chest injuries seen by clinicians is flail chest. This study aims to measure the overall mortality rate among flail chest patients and then to correlate mortality with several demographic, pathologic, and management factors.
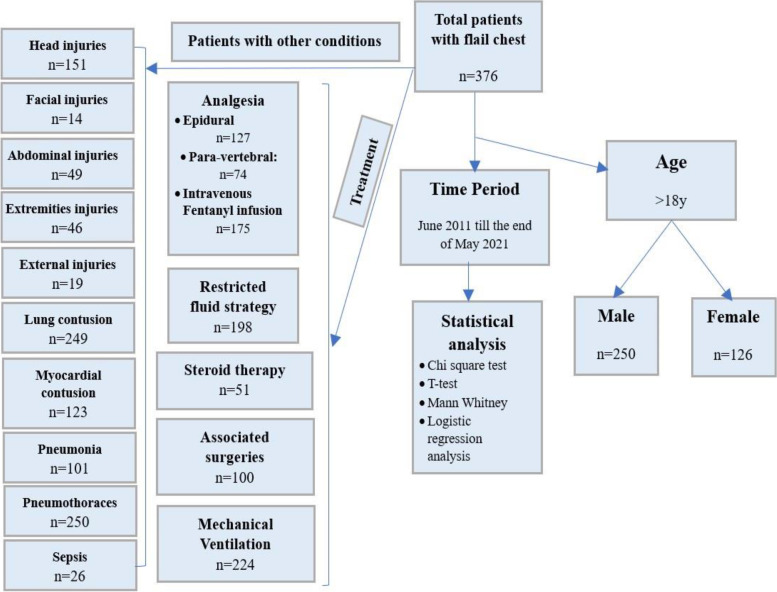
Methodology: A retrospective observational study tracked a total of 376 flail chest patients admitted to the emergency intensive care unit (EICU) and surgical intensive care unit (SICU) at Zagazig University over 120 months. The main outcome measurement was overall mortality. The secondary outcomes were the association of age and sex, concomitant head injury, lung and cardiac contusions, the onset of mechanical ventilation (MV) and chest tubes insertion, the length of mechanical ventilation and ICU stay in days, injury severity score (ISS), associated surgeries, pneumonia, sepsis, the implication of standard fluid therapy and steroid therapy, and the systemic and regional analgesia, with the overall mortality rates.
Results: The mortality rate was 19.9% overall. The shorter onset of MV and chest tube insertion, and the longer ICU, and hospital length of stay were noted in the mortality group compared with the survived group (P-value less than 0.05). Concomitant head injuries, associated surgeries, pneumonia, pneumothorax, sepsis, lung and myocardial contusion, standard fluid therapy, and steroid therapy were significantly correlated with mortality (P-value less than 0.05). MV had no statistically significant effect on mortality. Regional analgesia (58.8%) had a significantly higher survival rate than intravenous fentanyl infusion (41.2%). In multivariate analysis, sepsis, concomitant head injury, and high ISS were independent predictors for mortality [OR (95% CI) = 568.98 (19.49-16613.52), 6.86 (2.86-16.49), and 1.19 (1.09-1.30), respectively].
Conclusion: The current report recorded mortality of 19.9% between flail chest injury patients. Sepsis, concomitant head injury, and higher ISS are the independent risk factors for mortality when associated with flail chest injury. Considering restricted fluid management strategy and regional analgesia may help better outcome for flail chest injury patients.
Keywords: Flail chest; ICU; Morbidity; Mortality.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Alhadhrami B, Babsail A, Elhusseini M, Alhabboubi M, Chughtai TB. Traumatic flail chest injuries and the benefits of epidural analgesia. Clin Res Trial. 2017;3(2):1–5.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
