

Metabolic syndrome score as an indicator in a predictive nomogram for lymph node metastasis in endometrial cancer
- PMID: 37403054
- PMCID: PMC10318658
- DOI: 10.1186/s12885-023-11053-4
Metabolic syndrome score as an indicator in a predictive nomogram for lymph node metastasis in endometrial cancer
Abstract
Background: Lymph node metastasis (LNM) is an important factor affecting endometrial cancer (EC) prognosis. Current controversy exists as to how to accurately assess the risk of lymphatic metastasis. Metabolic syndrome has been considered a risk factor for endometrial cancer, yet its effect on LNM remains elusive. We developed a nomogram integrating metabolic syndrome indicators with other crucial variables to predict lymph node metastasis in endometrial cancer.
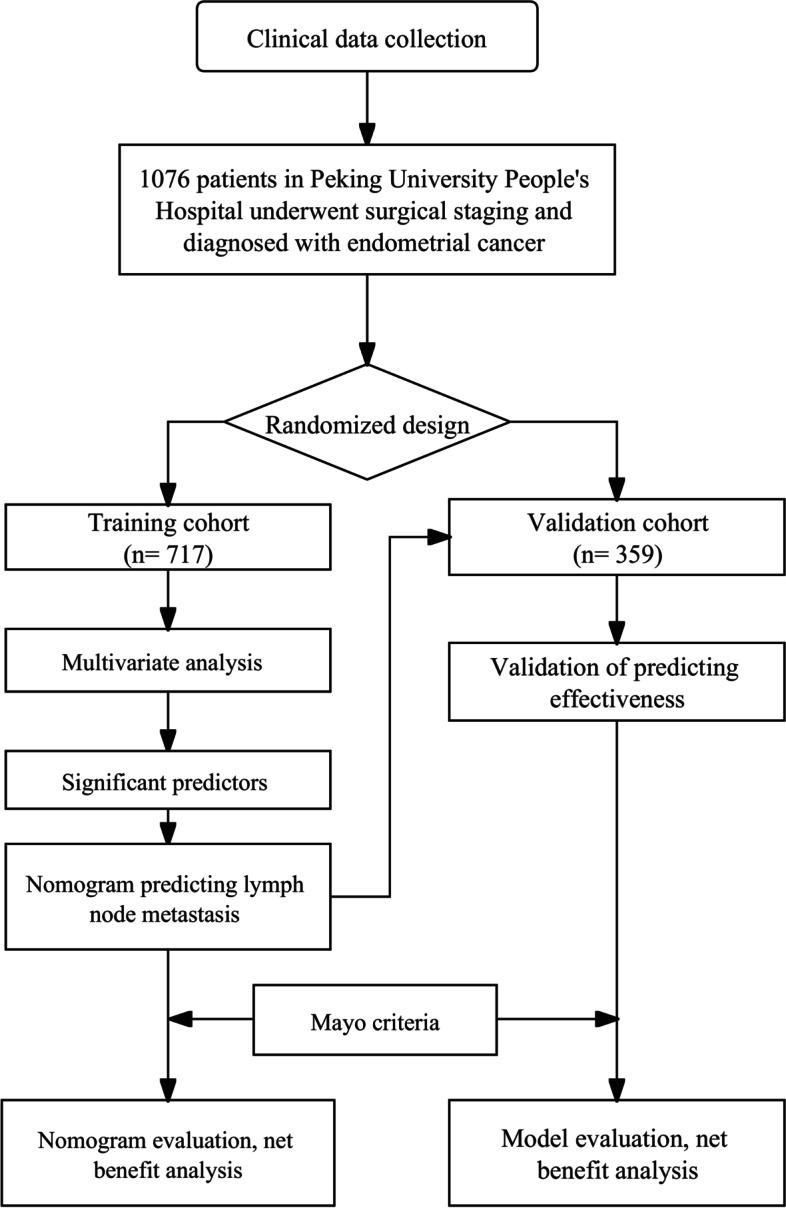
Methods: This study is based on patients diagnosed with EC in Peking University People's Hospital between January 2004 and December 2020. A total of 1076 patients diagnosed with EC and who underwent staging surgery were divided into training and validation cohorts according to the ratio of 2:1. Univariate and multivariate logistic regression analyses were used to determine the significant predictive factors.
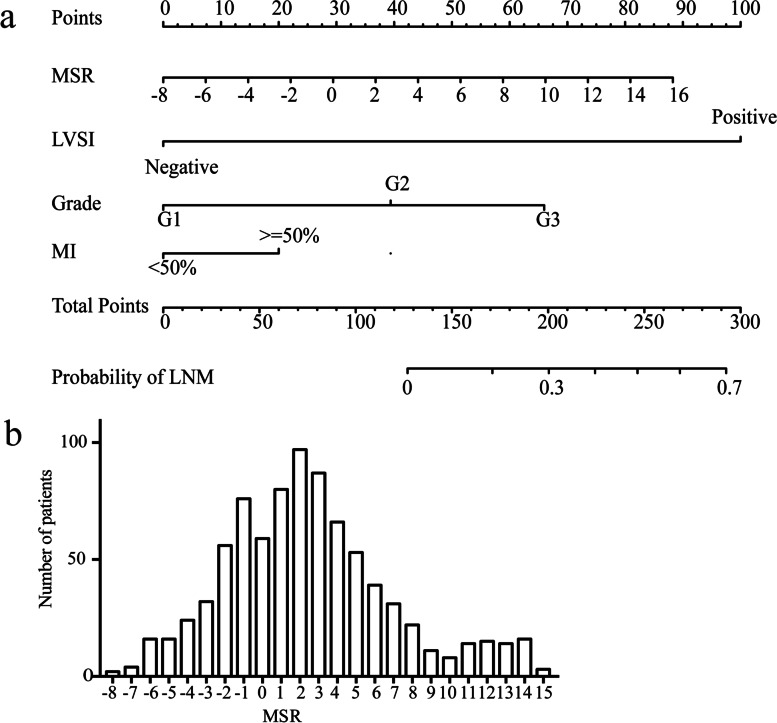
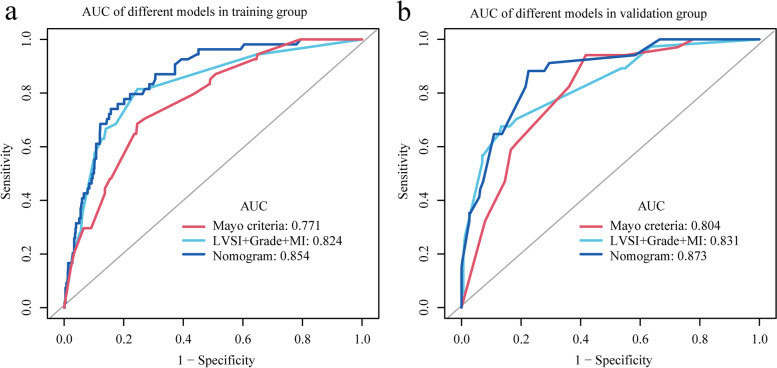
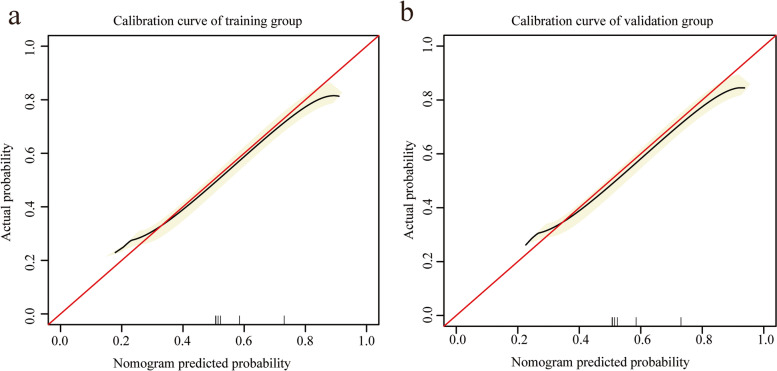
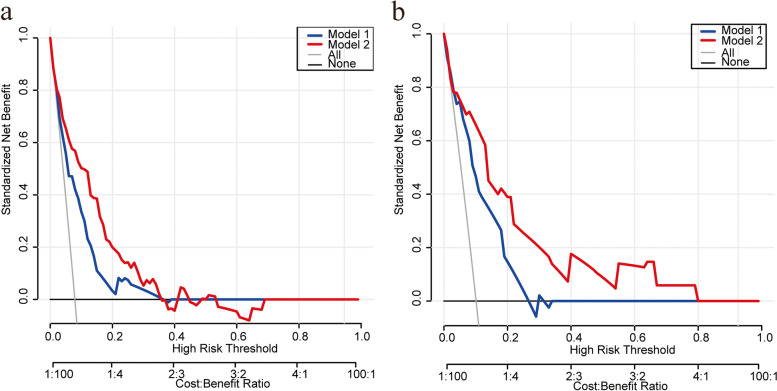
Results: The prediction nomogram included MSR, positive peritoneal cytology, lymph vascular space invasion, endometrioid histological type, tumor size > = 2 cm, myometrial invasion > = 50%, cervical stromal invasion, and tumor grade. In the training group, the area under the curve (AUC) of the nomogram and Mayo criteria were 0.85 (95% CI: 0.81-0.90) and 0.77 (95% CI: 0.77-0.83), respectively (P < 0.01). In the validation group (N = 359), the AUC was 0.87 (95% CI: 0.82-0.93) and 0.80 (95% CI: 0.74-0.87) for the nomogram and the Mayo criteria, respectively (P = 0.01). Calibration plots revealed the satisfactory performance of the nomogram. Decision curve analysis showed a positive net benefit of this nomogram, which indicated clinical value.
Conclusion: This model may promote risk stratification and individualized treatment, thus improving the prognosis.
Keywords: Endometrial cancer; Lymph node metastasis; Metabolic; Nomogram.
© 2023. The Author(s).
Conflict of interest statement
There is no conflict of interest to disclose.
Figures
Similar articles
-
Nomogram with potential clinical use to predict lymph node metastasis in endometrial cancer patients diagnosed incidentally by postoperative pathological assessment.Arch Gynecol Obstet. 2017 Oct;296(4):803-809. doi: 10.1007/s00404-017-4477-7. Epub 2017 Jul 31. Arch Gynecol Obstet. 2017. PMID: 28762064
-
A nomogram prediction model for lymph node metastasis in endometrial cancer patients.BMC Cancer. 2021 Jun 29;21(1):748. doi: 10.1186/s12885-021-08466-4. BMC Cancer. 2021. PMID: 34187416 Free PMC article.
-
[A nomogram for predicting lymph node metastasis in early gastric cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Jan 25;25(1):40-47. doi: 10.3760/cma.j.cn441530-20210208-00059. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35067033 Chinese.
-
Predictive models for lymph node metastasis in endometrial cancer: A systematic review and bibliometric analysis.Womens Health (Lond). 2024 Jan-Dec;20:17455057241248398. doi: 10.1177/17455057241248398. Womens Health (Lond). 2024. PMID: 38725247 Free PMC article.
-
A prediction nomogram for postoperative gastroparesis syndrome in right colon cancer: a retrospective study.Langenbecks Arch Surg. 2023 Apr 13;408(1):148. doi: 10.1007/s00423-023-02885-6. Langenbecks Arch Surg. 2023. PMID: 37052749 Review.
Cited by
-
circRNAs in Endometrial Cancer-A Promising Biomarker: State of the Art.Int J Mol Sci. 2024 Jun 9;25(12):6387. doi: 10.3390/ijms25126387. Int J Mol Sci. 2024. PMID: 38928094 Free PMC article. Review.
-
Association Between Hepatic Steatosis Index and Endometrial Cancer Risk: A Cross-Sectional Study.Int J Womens Health. 2025 Mar 17;17:825-833. doi: 10.2147/IJWH.S497621. eCollection 2025. Int J Womens Health. 2025. PMID: 40123758 Free PMC article.
-
Use of clinical variables for preoperative prediction of lymph node metastasis in endometrial cancer.Jpn J Clin Oncol. 2024 Jan 7;54(1):38-46. doi: 10.1093/jjco/hyad135. Jpn J Clin Oncol. 2024. PMID: 37815156 Free PMC article.
References
-
- Morrow CP, Bundy BN, Homesley HD, et al. Doxorubicin as an adjuvant following surgery and radiation therapy in patients with high-risk endometrial carcinoma, stage I and occult stage II: a Gynecologic Oncology Group Study. Gynecol Oncol. 1990;36(2):166–171. doi: 10.1016/0090-8258(90)90166-I. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
