

Personalized nutrition therapy in critical care: 10 expert recommendations
- PMID: 37403125
- PMCID: PMC10318839
- DOI: 10.1186/s13054-023-04539-x
Personalized nutrition therapy in critical care: 10 expert recommendations
Abstract
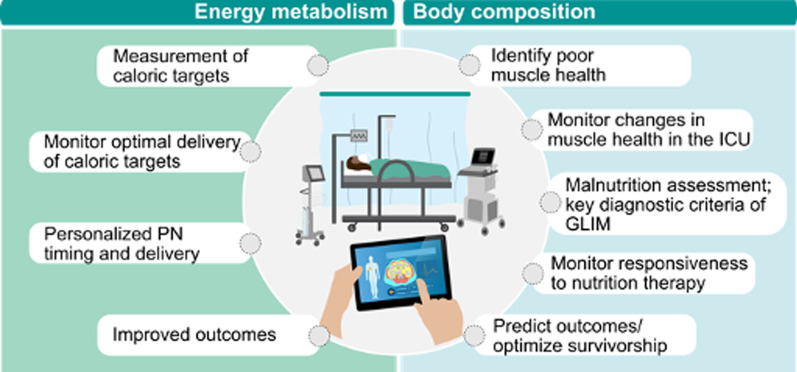
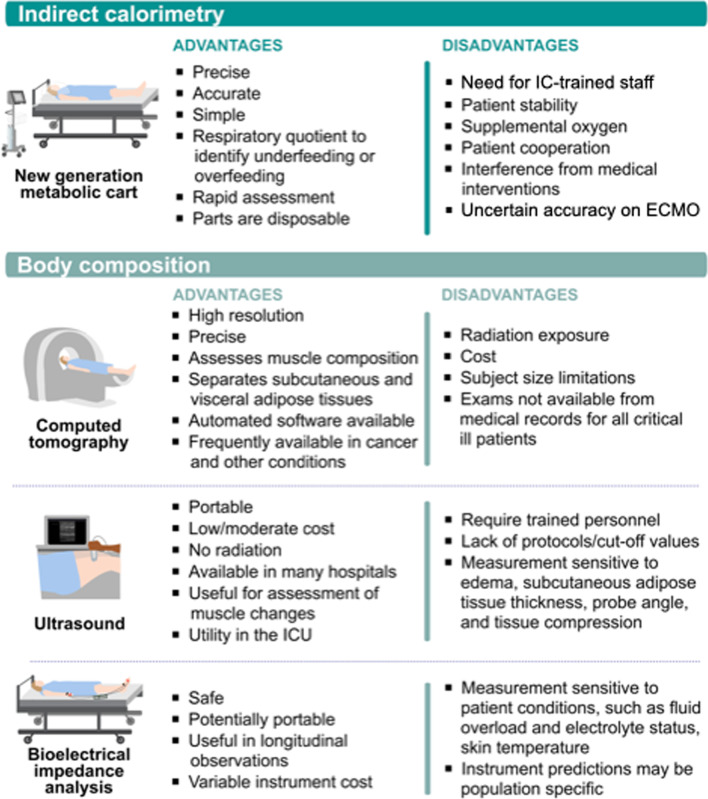
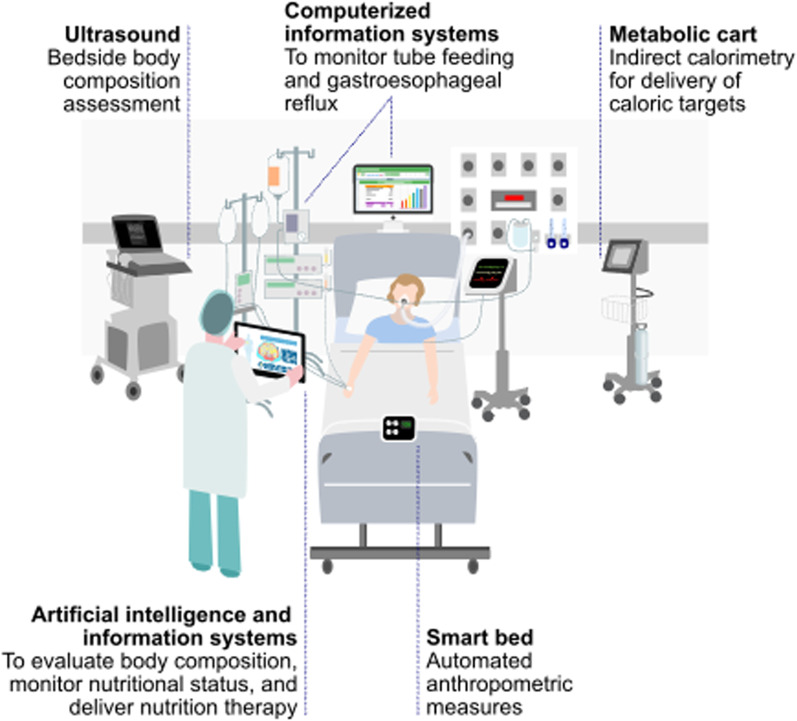
Personalization of ICU nutrition is essential to future of critical care. Recommendations from American/European guidelines and practice suggestions incorporating recent literature are presented. Low-dose enteral nutrition (EN) or parenteral nutrition (PN) can be started within 48 h of admission. While EN is preferred route of delivery, new data highlight PN can be given safely without increased risk; thus, when early EN is not feasible, provision of isocaloric PN is effective and results in similar outcomes. Indirect calorimetry (IC) measurement of energy expenditure (EE) is recommended by both European/American guidelines after stabilization post-ICU admission. Below-measured EE (~ 70%) targets should be used during early phase and increased to match EE later in stay. Low-dose protein delivery can be used early (~ D1-2) (< 0.8 g/kg/d) and progressed to ≥ 1.2 g/kg/d as patients stabilize, with consideration of avoiding higher protein in unstable patients and in acute kidney injury not on CRRT. Intermittent-feeding schedules hold promise for further research. Clinicians must be aware of delivered energy/protein and what percentage of targets delivered nutrition represents. Computerized nutrition monitoring systems/platforms have become widely available. In patients at risk of micronutrient/vitamin losses (i.e., CRRT), evaluation of micronutrient levels should be considered post-ICU days 5-7 with repletion of deficiencies where indicated. In future, we hope use of muscle monitors such as ultrasound, CT scan, and/or BIA will be utilized to assess nutrition risk and monitor response to nutrition. Use of specialized anabolic nutrients such as HMB, creatine, and leucine to improve strength/muscle mass is promising in other populations and deserves future study. In post-ICU setting, continued use of IC measurement and other muscle measures should be considered to guide nutrition. Research on using rehabilitation interventions such as cardiopulmonary exercise testing (CPET) to guide post-ICU exercise/rehabilitation prescription and using anabolic agents such as testosterone/oxandrolone to promote post-ICU recovery is needed.
Keywords: Body composition; Critical illness; Enteral nutrition; ICU; Indirect calorimetry; Micronutrients; Muscle; Nutrition; Parenteral nutrition; Protein; TPN; Testosterone.
© 2023. The Author(s).
Conflict of interest statement
Prof. Wischmeyer reports receiving investigator-initiated grant funding related to this work from the National Institutes of Health, Department of Defense, Abbott, Baxter, and Fresenius. Dr. Wischmeyer has served as a consultant to Abbott, Fresenius, Baxter, Mend Inc, and Nutricia for research related to this work. Dr. Wischmeyer received unrestricted gift donations for nutrition research from Musclesound and DSM. Dr. Wischmeyer has received honoraria or travel expenses for CME lectures on improving nutrition care from Abbott, Baxter, Fresenius, Danone-Nutricia, DSM, and Nestle. Prof. Dr. Van Zanten reported receiving honoraria for advisory board meetings, lectures, research, and travel expenses from AOP Pharma, Baxter, Cardinal Health, Danone-Nutricia, DIM3, Fresenius Kabi, GE Healthcare, Mermaid, Rousselot, and Lyric. Prof Mette M Berger received honoraria for lectures on nutrition therapy from Abbott, Baxter, Fresenius Kabi, DSM, and Nestle Health Science. Prof. Dr. Elisabeth De Waele reports receiving investigator-initiated grant funding related to her work from the Belgian National Institutes of Health, Federaal Kennis Centrum, Wetenschappelijk Fonds Willy Gepts, Baxter Healthcare, Danone-Nutricia and Fresenius. She reports receiving honoraria for advisory board meetings, lectures, research, and travel expenses from Baxter Healthcare, Cardinal Health, Danone-Nutricia, Fresenius Kabi, and ARTMedical. Dr Puthucheary reports receiving honoraria for advisory board meetings and lectures from Fresenius Kabi, Nestle, Baxter, Nutricia and Faraday Pharmaceuticals, and research funding from Baxter and Nestle. Dr. Bear reports receiving honoraria for advisory board meetings from Avanos, Cardinal Health and Nutricia and lectures from Baxter and Cardinal Health. Prof Prado has previously received honoraria and/or paid consultancy from Abbott Nutrition, Nutricia, Nestlé Health Science, Fresenius Kabi, AMRA Medical, and Pfizer. Outside of the submitted work, Dr. Ridley reports unrestricted grants paid to my institution from Baxter Healthcare (USA), Nutricia Australia and Fresenius Kabi Australia and personal fees for speaking from Nestle Australia, Baxter Healthcare (USA), Baxter Healthcare (Australia), Nutricia Australia, Fresenius Kabi and Nestle Australia. Dr Ridley has salary support from National Health and Medical Research Council HMRC Emerging Leadership Investigator Grant.
Figures

References
-
- McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, McCarthy MS, Davanos E, Rice TW, Cresci GA, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically Ill patient: society of critical care medicine (SCCM) and American society for parenteral and enteral nutrition (ASPEN) JPEN J Parenter Enteral Nutr. 2016;40(2):159–211. doi: 10.1177/0148607115621863. - DOI - PubMed
-
- Elke G, Hartl WH, Kreymann KG, Adolph M, Felbinger TW, Graf T, de Heer G, Heller AR, Kampa U, Mayer K, et al. Clinical nutrition in critical care medicine—guideline of the German society for nutritional medicine (DGEM) Clin Nutr ESPEN. 2019;33:220–275. doi: 10.1016/j.clnesp.2019.05.002. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
