

Learning Curve and Clinical Outcomes of Ultrasonic Osteotome-based En Bloc Laminectomy for Thoracic Ossification of the Ligamentum Flavum
- PMID: 37403615
- PMCID: PMC10475665
- DOI: 10.1111/os.13804
Learning Curve and Clinical Outcomes of Ultrasonic Osteotome-based En Bloc Laminectomy for Thoracic Ossification of the Ligamentum Flavum
Abstract
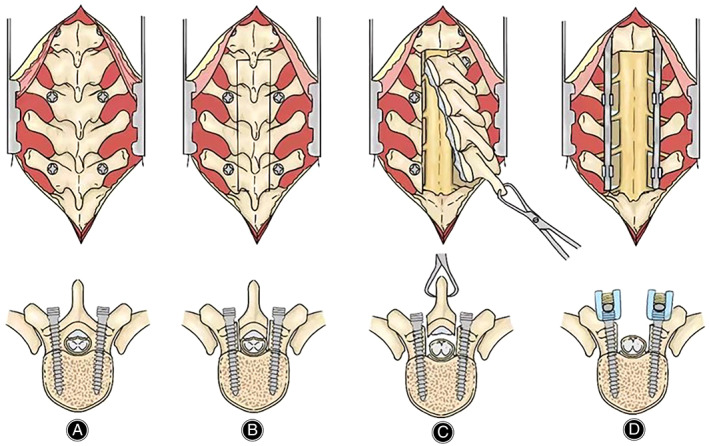
Objective: Despite rapid advances in minimally invasive surgery, en bloc laminectomy remains the most common surgical approach for treating thoracic ossification of the ligamentum flavum (TOLF). However, the learning curve of this risky operation is rarely reported. Therefore, we aimed to describe and analyze the learning curve of ultrasonic osteotome-based en bloc laminectomy for TOLF.
Methods: Among 151 consecutive patients with TOLF who underwent en bloc laminectomy performed by one surgeon between January 2012 and December 2017, we retrospectively analyzed their demographic data, surgical parameters, and neurological function. Neurological outcome was evaluated with the modified Japanese Orthopaedic Association (mJOA) scale, and the Hirabayashi method was used to calculate the neurological recovery rate. The learning curve was assessed with logarithmic curve-fitting regression analysis. Univariate analysis methods were used for statistical analysis, including t-test, rank sum test, and chi-square test.
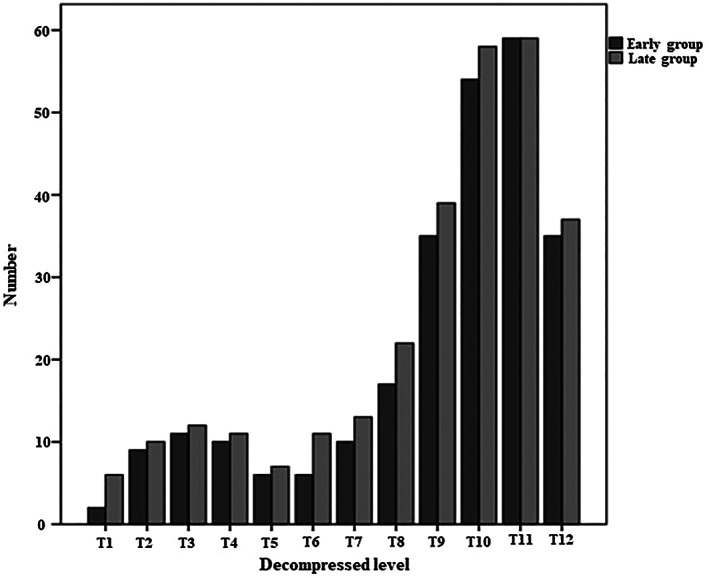
Results: A total of 50% of learning milestones could be reached in approximately 14 cases, and the asymptote in 76 cases. Therefore, 76 of the 151 enrolled patients were defined as the "early group," and the remaining 75 were delimitated as the "late group" for comparison. There was a significant intergroup difference in the corrected operative time (94.80 ± 27.77 vs 65.93 ± 15.67 min, P < 0.001) and the estimated blood loss (median 240 vs 400 mL, P < 0.001). The overall follow-up was 83.1 ± 18.5 months. The mJOA significantly increased from a median of 5 (IQR: 4-5) before the surgery to 10 (IQR: 9-10) at the last follow-up (P < 0.001). The overall complication rate was 37.1%, and no significant intergroup difference was found, except for the incidence of dural tears (31.6% vs 17.3%, p = 0.042).
Conclusion: Initially, mastering the en bloc laminectomy technique using ultrasonic osteotome for TOLF treatment can be challenging, but the surgeon's experience improves as the operative time and blood loss decrease. Improved surgical experience reduced the risk of dural tears but was not associated with the overall complication rate or long-term neurological function. Despite the relatively long learning curve, en bloc laminectomy is a secure and valid technique for TOLF treatment.
Keywords: En Bloc Laminectomy; Learning Curve; Thoracic Ossification of the Ligamentum Flavum; Ultrasonic Osteotome.
© 2023 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors have no further conflicts of interest to report.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
