

Should Core Needle Lymph Node Biopsy be a Relevant Alternative to Surgical Excisional Biopsy in Diagnostic Work Up of Lymphomas?
- PMID: 37403909
- PMCID: PMC10440969
- DOI: 10.5152/eurasianjmed.2023.0060
Should Core Needle Lymph Node Biopsy be a Relevant Alternative to Surgical Excisional Biopsy in Diagnostic Work Up of Lymphomas?
Abstract
Objective: Surgical excisional biopsy is accepted as the standard of care approach in the diagnosis of lympho- mas. Financial issues related to the increased cost and the invasive nature of the procedure forced physicians to use some alternative diagnostic methods. Percutaneous core needle biopsy, which gained a reputation for the diagnosis of lymphomas with the advent of improved pathological, immunohistochemical, and molecular analysis, made it possible to have an accurate diagnosis with limited tissue samples. In this retrospective study, we aimed to compare the diagnostic yield of surgical excisional biopsy and core needle biopsy.
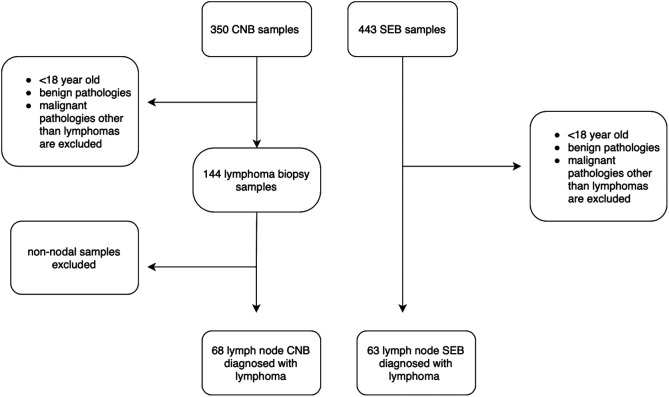
Materials and methods: This study included 131 patients who were diagnosed with lymphoma with a nodal biopsy which was acquired via surgical excisional biopsy or core needle biopsy between 2014 and 2020 in our center. Around 68 patients underwent surgical excisional biopsy and the remaining 63 underwent core needle biopsy. Samples that allowed to the identification of the exact tumor type and/or subtype were accepted as fully diagnostic. Sufficient amount of tissue that the pathologist could have any suspicious findings considering malignant lymphoma was classified as partial diagnostic group. Inadequate samples were the ones who were not enough to report any final diagnosis.
Results: The patients who underwent a core needle biopsy were significantly older than the patients who underwent to surgical excisional biopsy (56.8 vs. 47.6, P = .003). Despite the full diagnostic ability of surgical excisional biopsy outperformed core needle biopsy (95.2 % vs. 83.8 %, P=.035), in 92.6% of the patients whose tissue samples were obtained via core needle biopsy were accepted to have a sufficient diagnosis to initiate the treatment and not required a second biopsy, which was comparable with the ones achieved by surgical excisional biopsy (92.6% vs. 95.2%, P = .720).
Conclusion: According to the results obtained in our study, we may conclude that core needle biopsy is a viable and comparable alternative to surgical excisional biopsy, offering a less invasive and less-expansive approach.
Figures
References
-
- Swerdlow SH, Campo E, Harris N.et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. WHO; 2017;2.
LinkOut - more resources
Full Text Sources