

Correct Closure of the Left Atrial Appendage Reduces Stagnant Blood Flow and the Risk of Thrombus Formation: A Proof-of-Concept Experimental Study Using 4D Flow Magnetic Resonance Imaging
- PMID: 37404107
- PMCID: PMC10323417
- DOI: 10.3348/kjr.2023.0173
Correct Closure of the Left Atrial Appendage Reduces Stagnant Blood Flow and the Risk of Thrombus Formation: A Proof-of-Concept Experimental Study Using 4D Flow Magnetic Resonance Imaging
Abstract
Objective: The study was conducted to investigate the effect of correct occlusion of the left atrial appendage (LAA) on intracardiac blood flow and thrombus formation in patients with atrial fibrillation (AF) using four-dimensional (4D) flow magnetic resonance imaging (MRI) and three-dimensional (3D)-printed phantoms.
Materials and methods: Three life-sized 3D-printed left atrium (LA) phantoms, including a pre-occlusion (i.e., before the occlusion procedure) model and correctly and incorrectly occluded post-procedural models, were constructed based on cardiac computed tomography images from an 86-year-old male with long-standing persistent AF. A custom-made closed-loop flow circuit was set up, and pulsatile simulated pulmonary venous flow was delivered by a pump. 4D flow MRI was performed using a 3T scanner, and the images were analyzed using MATLAB-based software (R2020b; Mathworks). Flow metrics associated with blood stasis and thrombogenicity, such as the volume of stasis defined by the velocity threshold (|V̅| < 3 cm/s), surface-and-time-averaged wall shear stress (WSS), and endothelial cell activation potential (ECAP), were analyzed and compared among the three LA phantom models.
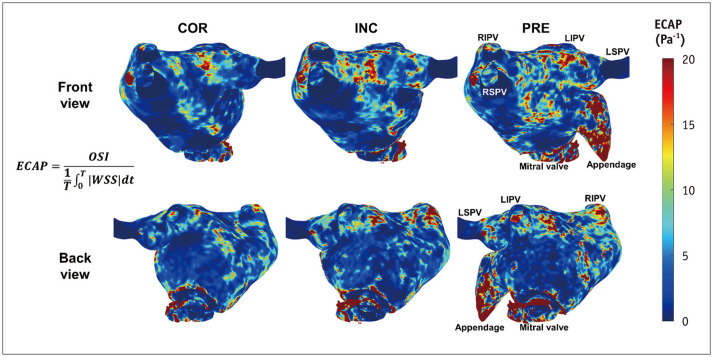
Results: Different spatial distributions, orientations, and magnitudes of LA flow were directly visualized within the three LA phantoms using 4D flow MRI. The time-averaged volume and its ratio to the corresponding entire volume of LA flow stasis were consistently reduced in the correctly occluded model (70.82 mL and 39.0%, respectively), followed by the incorrectly occluded (73.17 mL and 39.0%, respectively) and pre-occlusion (79.11 mL and 39.7%, respectively) models. The surface-and-time-averaged WSS and ECAP were also lowest in the correctly occluded model (0.048 Pa and 4.004 Pa-1 , respectively), followed by the incorrectly occluded (0.059 Pa and 4.792 Pa-1 , respectively) and pre-occlusion (0.072 Pa and 5.861 Pa-1 , respectively) models.
Conclusion: These findings suggest that a correctly occluded LAA leads to the greatest reduction in LA flow stasis and thrombogenicity, presenting a tentative procedural goal to maximize clinical benefits in patients with AF.
Keywords: 4D flow MRI; Atrial fibrillation; Hemodynamics; Left atrial appendage occlusion; Stasis; Thrombogenicity.
Copyright © 2023 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures






References
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. - PubMed
-
- Holmes DR, Jr, Lakkireddy DR, Whitlock RP, Waksman R, Mack MJ. Left atrial appendage occlusion: opportunities and challenges. J Am Coll Cardiol. 2014;63:291–298. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–2962. - PubMed
-
- Blackshear JL, Odell JA. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann Thorac Surg. 1996;61:755–759. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
